Adenoid Cystic Carcinoma of Thyroid - Unusual Primary Site and Diagnostic Considerations in Cytology
Adenoid Cystic Carcinoma of Thyroid - Unusual Primary Site and Diagnostic Considerations in Cytology
Vijayalakshmi Gudivada MD FRCpath1*, Parepalli Divya MD1, Pampa ch Toi MD1, Sreekanth Gaddam MBBS, MSc2
1. Department of Pathology, Jawaharlal Institute of Postgraduate Medical Education & Research ( JIPMER) Puducherry, India.
2. MSc Internal medicine, University of Edinburgh, Scotland, United Kingdom.
*Correspondence to: Vijayalakshmi Gudivada, Specialist Clinical and anatomic pathologist, Premier diagnostic center, Prime healthcare group, Dubai, United Arab Emirates.
Copyright
© 2024 Vijayalakshmi Gudivada. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 14 November 2024
Published: 23 November 2024
DOI: https://doi.org/10.5281/zenodo.14208205
Abstract
Adenoid cystic carcinoma (ACC) is a rare head and neck tumor, typically arising from both major and minor salivary glands and sweat gland epithelium. This case report presents a 38-year-old female with primary thyroid ACC, an exceedingly rare entity with only a very few cases reported in the literature. The patient presented with a solitary thyroid nodule, Fine needle aspiration cytology revealed basaloid cells in three-dimensional clusters with many luminal hyaline globules, consistent with ACC. Immunohistochemistry supported the diagnosis by demonstrating CD117 positivity and subsequent histopathology confirmed ACC limited to the thyroid without extrathyroidal extension. ACC, characterized by perineural invasion and late distant metastasis, necessitates thorough clinicoradiological assessments to rule out direct extension or metastasis from adjacent structures into thyroid gland before considering primary from thyroid. Differential diagnoses, such as adenoid cystic variant of papillary thyroid carcinoma, require careful cytological observation. ACC treatment involves complete surgical excision, and postoperative radiotherapy may be considered in cases with perineural invasion or high-grade tumors. This case highlights the importance of fine needle aspiration cytology and immunohistochemistry in diagnosing primary thyroid ACC , emphasizing the need for differentiation from other thyroid tumors with similar morphology and direct thyroid invasion from neighbouring structures. Given its rarity, the establishment of standard treatment protocols for primary thyroid ACC remains challenging, underscoring the importance of long-term follow-up and consideration of adjuvant radiotherapy in certain cases.
Keywords: Cytology, adenoid cystic carcinoma, hyaline globules, thyroid nodule, fine needle aspiration cytology.
Adenoid Cystic Carcinoma of Thyroid - Unusual Primary Site and Diagnostic Considerations in Cytology
LIST OF ABBREVIATIONS
ACC - Adenoid cystic carcinoma
CECT - Contrast Enhanced Computerized Tomography
FNAC - Fine needle aspiration cytology
H&E- Hematoxylin and Eosin
IHC- Immunohistochemistry
ORR- Overall response rate
TTF1- Thyroid transcription Factor- 1
USG- Ultrasonography
Introduction
Adenoid cystic carcinoma (ACC) is a rare head and neck tumor occurring at a frequency of less than 0.2/million.1 It typically originates from major and minor salivary gland and sweat gland epithelium in skin and breast and upto 90% ACCs show MYB-NFIB or MYBL1-NFIB fusion and are characterized by a slow-growing nature but possess local aggressiveness due to their tendency for perineural invasion, often resulting in late distant metastasis. These tumors are predominantly seen in individuals aged between their fifth and sixth decades, with a slight female predominance. Although ACC primarily affects salivary glands, it can also manifest in extra glandular sites such as the trachea, lung, upper anterior mediastinum,2 esophagus, and cervix, sharing similar morphological characteristics with salivary gland tumors. Due to its propensity for local infiltration from adjacent structures, ACC may present as swelling in the thyroid.3,4,5 Primary thyroid adenoid cystic carcinoma is an exceedingly rare entity, with only few documented cases reported in the literature to date. This article presents a case report of primary thyroid ACC diagnosed via fine needle aspiration followed by histopathology correlation.
Case Presentation
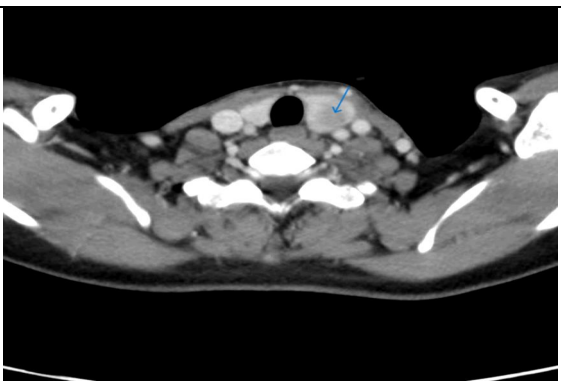
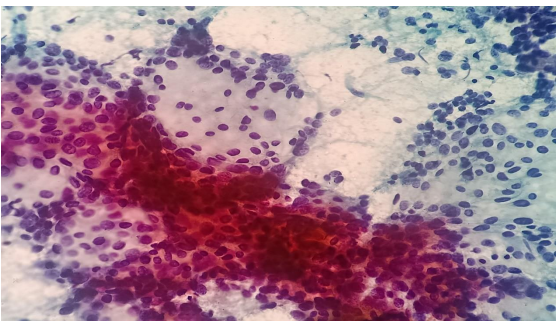
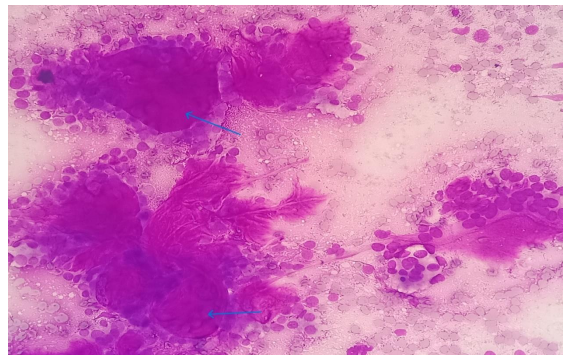
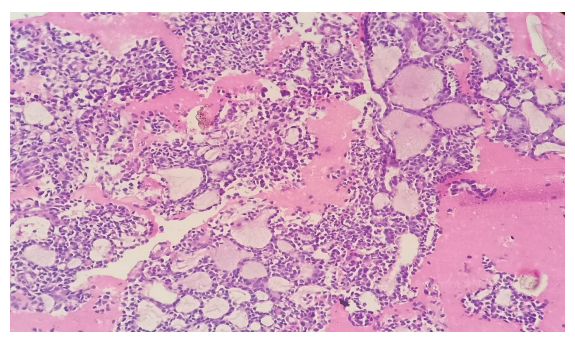
A 38 year old female presented with the complaints of pain and difficulty during swallowing and history of weight loss. Up on examination, a swelling was noted on the left side of her neck, which moved with deglutition. Ultrasound (USG) revealed a well circumscribed hypoechoic nodule measuring 3.2x2.1cm in the left lobe of thyroid with no extrathyroidal extension, however the nodule was compressing the esophagus. Fine needle aspiration was performed on the lesion and stained with Papanicolaou (PAP) stain and May Grunwald Geimsa (MGG) stains. The smears exhibited high cellularity with globoid clusters and three dimensional tissue fragments composed of aggregates of cells with central core of homogenous basement membrane material with cells having basaloid morphology and scant cytoplasm (Figure 2). MGG smears highlighted pink/ magenta amorphous basement membrane hyaline globules in the clusters of tumor cells (Figure 3). Cell block preparation of fine needle aspiration showed cribriform pattern of tumor cells with hyaline globules (Figure 4). Immunocytochemistry conducted on cell block shows TTF-1 positivity in normal thyroid follicles and negative staining in tumor cell clusters. CD117 and synaptophysin were inconclusive on cell block, but based on morphology this case was reported as adenoid cystic carcinoma of thyroid. Contrast-enhanced computed tomography (CECT) prior to surgery depicted a well defined heterogeneously enhancing hypodense lesion in the left lobe of thyroid measuring 3.2x2.1x1.7cm with no additional lesions or abnormalities noted in the adjacent structures like trachea, larynx, oesophagus or upper mediastinum(Figure 1). The excised left hemi-thyroidectomy specimen was received which showed a grey white solid homogenous lesion measuring 3.5x2.2x2cm reaching till the capsule. No cystic spaces/papillary projections/colloid seen in the lesion grossly. Adjacent thyroid parenchyma was normal. Histopathology sections showed tumor arranged in tubules and cribriform pattern along with hyaline globules suggesting the diagnosis of adenoid cystic carcinoma of thyroid, limited to thyroid without extra thyroid extension (Figure 5). IHC with CD117 showed cytoplasmic positivity in tumor cells further supporting the diagnosis (Figure 6).
Figure 1: Contrast-enhanced computed tomography of neck with well defined heterogeneously enhancing hypodense lesion in left lobe, limited to thyroid (arrow).
Figure 2: Papanicoalaou stained (20x) showing globoid clusters of basaloid cells with luminal hyaline globules.
Figure 3: MGG stained smears (20x) showing globoid clusters of basaloid cells with luminal hyaline globules(arrow).
Figure 4: H &E section from Cell block preparation of fine needle aspiration (20x) showing cribriform pattern of tumor cells with hyaline globules.
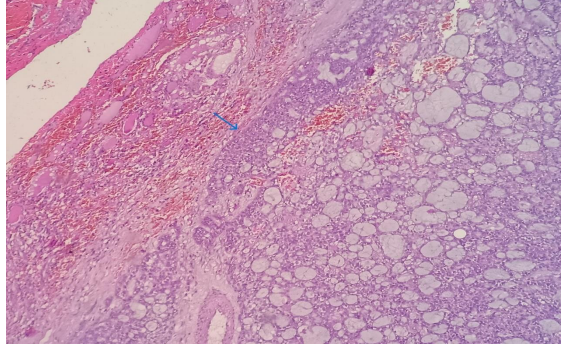
Figure 5: H & E section from Left hemithyroidectomy specimen (20x) show well circumscribed tumor with features of adenoid cystic carcinoma, limited to thyroid with adjacent normal thyroid parenchyma (Arrow marks the junction of tumor with normal thyroid parenchyma).
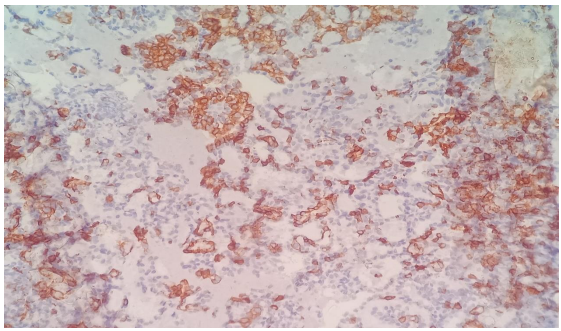
Figure 6: IHC stain (20x) showing cytoplasmic positivity of CD117 in tumor cells.
Discussion
Adenoid cystic carcinoma (ACC) is a rare tumor, predominantly found in minor salivary glands, although it can also originate from submucosal glands of the larynx, trachea, and lungs. No significant predisposing factors have been identified for this malignancy.6 Cytologically, ACCs are biphasic tumors with both epithelial and myoepithelial components, characterized by cohesive clusters of monomorphic epithelial cells with a high nuclear/cytoplasmic ratio, round nuclei, coarse chromatin, prominent nucleoli, and scant cytoplasm. Additionally, characteristic globules of homogenous, acellular hyaline material are observed alongside cellular elements, with dispersed naked nuclei in the background. ACC presents in three morphological variants, with tubular and cribriform patterns associated with a good prognosis, while a solid pattern shows more aggressive behaviour.6 Upto date, only two articles have reported primary thyroid ACC, one as a letter to the editor8 and other publication as a literature review of few other cases.9
While there are documented cases of ACC variants coexisting with papillary carcinoma of the thyroid or ACC originating from the larynx or minor salivary glands rarely extending into the thyroid and presenting as thyroid nodule, which needs to be ruled out before diagnosing primary thyroid ACC.1,5,7 Complete clinico-radiological evaluation is required to rule out local infiltration of either ACC from larynx/ trachea or locally aggressive Thyroid Anaplastic carcinoma.9 When presented as thyroid nodule, fine needle aspiration is the most feasible, safe, and cost-effective method for initial diagnosis. Careful observation of cytological features is crucial to avoid possibility of misdiagnosis on FNA smears, particularly in distinguishing ACC from other thyroid tumors like papillary thyroid carcinoma or follicular neoplasm.These diagnostic pitfalls can be avoided by cytological features like cell type, architectural pattern, chromatin pattern. Presence of nuclear grooves, intra-nuclear inclusions and papillary or micro-follicular pattern suggests diagnosis of papillary thyroid carcinoma/ follicular neoplasm.10 Ropy colloid can be mistaken for hyaline globules. The other differential diagnosis can be adenoid cystic variant of papillary carcinoma of thyroid11 which was described as a rare variant in the literature and show nuclear features of papillary carcinoma in micro-follicular pattern or cribriform pattern with hyaline globules seen in the background instead of ropy colloid. Immunohistochemistry helps in diagnosing this rare variant, which shows thyroglobulin positivity in tumor cells but negative staining in hyaline globules. In this variant hyaline globules may be arising from psammoma bodies.12 In some instances, hyaline globules can be mistaken for amyloid leading to misdiagnosis of medullary carcinoma, in these cases typical salt and pepper chromatin pattern and immunohistochemistry with calcitonin are to be considered to rule out medullary carcinoma.8 Poorly differentiated thyroid carcinoma can show residual microfollicles with hyaline globules mimicking ACC.3 Proper cytomorphological evaluation and TTF1, Pax-8 and Thyroglobulin positivity on immunohistochemistry can rule out ACC. Differentiation from other primary thyroid tumors with similar morphology, such as Cribriform morular thyroid carcinoma and Hyalinizing trabecular tumor14 is essential, as ACC requires long-term follow-up due to its propensity for perineural invasion and hematogenous spread. In our case, tumor was a solitary thyroid nodule, limited to thyroid and both cytology smears and histopathology sections lacked nuclear features of papillary thyroid carcinoma and showed typical morphological features of ACC, and positive CD117 staining on immunohistochemistry, further supported the diagnosis of primary thyroid adenoid cystic carcinoma. In general ACC show positivity for smooth muscle actin, P63, CD117, P53 and BCL2 and show characteristic t(6,9) MYB-NFIB fusion and will be negative for Thyroglobulin, Pax-8 and TTF1.9
As treatment protocols for primary thyroid ACC are lacking, complete surgical excision is considered effective. Postoperative radiotherapy may be warranted in cases of frequent perineural invasion, positive margins, metastatic disease, or high-grade tumors to reduce local recurrence.14,15 Targeted therapies against the cKIT receptor using tyrosine kinase inhibitors were one of the first attempts of precision therapy in patients with ACC, specifically using imatinib, dasatinib, or sunitinib therapy. Unfortunately, while high cKIT expression in ACC has been well established, these studies were largely disappointing, with an overall response rate (ORR) below 5% and no significant improvement in patient survival in any of these trials16.
Conclusion
Although primary thyroid adenoid cystic carcinoma is exceptionally rare, it can be accurately diagnosed using a cost effective and safe method of fine needle aspiration cytology combined with immunocytochemistry. However, it is crucial to differentiate it from the adenoid cystic variant or follicular variant of papillary thyroid carcinoma, as well as other primary thyroid tumors with similar morphology. Complete clinico-radiological evaluation is necessary to rule out direct extension or metastasis of ACC from neighboring structures before considering the possibility of primary thyroid ACC. Given the close proximity of the thyroid to laryngeal nerves, primary thyroid ACC often exhibits frequent perineural invasion, leading to local recurrences and metastases, necessitating long-term follow-up and potentially postoperative radiotherapy.
ACKNOWLEDGEMENT
We acknowledge the Department of Surgery for their contribution to the management of this case.
COMPETING INTEREST STATEMENT BY ALL AUTHORS
There is no competing interest from any of the authors.
AUTHORSHIP STATEMENT BY ALL AUTHORS
Dr. Vijayalakshmi and Dr. Divya -Collection of data and preparation of the manuscript including histopathology, imaging, and review of the manuscript. Dr. Pampa- Review of the manuscript and cytodiagnosis. Dr. Sreekanth Gaddam- Proof reading and editing. All authors have contributed to the diagnosis, management and the manuscript preparation.
ETHICS STATEMENT BY ALL AUTHORS
Consent was obtained for FNAC and permission was obtained for publication. No identification details of the patient are disclosed.
References
1. Jikuzono, Tomoo & Suzuki, Shigekazu & Ishibashi, Osamu & Kure, Shoko & Sakanushi, Atsuko & Nakamizo, Munenaga & Kawamoto, Masashi & Ohashi, Ryuji & Yamada, Tetsu & Sugitani, Iwao. (2021). Clinical Utility of Fine Needle Aspiration Cytology for Adenoid Cystic Carcinoma of the Trachea with Thyroid Invasion: A Case Report. Journal of Nippon Medical School. 89. 10.1272/jnms.JNMS.2022_89-207.
2. Wu Q, Sun W, Bu J, Xiang Y, Zhong Y. Primary Adenoid Cystic Carcinoma of the Upper Anterior Mediastinum Mimicking a Thyroid Tumor: A Case Report and Review of Literature. Front Endocrinol (Lausanne). 2020 Apr 23;11:242. doi: 10.3389/fendo.2020.00242. PMID: 32390945; PMCID: PMC7191109.
3. Qi D, Feng L, Li J, Liu B, Zhang Q. Primary adenoid cystic carcinoma of the trachea with thyroid invasion: a case report and literature review. Onco Targets Ther. 2016 Oct 13;9:6291-6296. doi: 10.2147/OTT.S112498. PMID: 27785076; PMCID: PMC5066988.
4. Nuwal P, Dixit R, Singhal AK. Primary adenoid cystic carcinoma of trachea presenting as midline neck swelling and mimicking thyroid tumor: A case report and review of literature. Lung India. 2010 Jul;27(3):167-9. doi: 10.4103/0970-2113.68330. PMID: 20931039; PMCID: PMC2946722.
5. Rocca BJ, Barone A, Ginori A, Ambrosio MR, Disanto A. Unusual presentation of metastatic adenoid cystic carcinoma: a challenge in aspiration cytology of the thyroid. Pathologica. 2014 Dec;106(4):342-4. PMID: 25845052.
6. Mandal S, Jain S. Adenoid cystic pattern in follicular variant of papillary thyroid carcinoma: a report of four cases. Cytopathology. 2010 Apr;21(2):93-6. doi: 10.1111/j.1365-2303.2009.00654.x. Epub 2009 May 14. PMID: 19456847.
7. Idowu MO, Reiter ER, Powers CN. Adenoid cystic carcinoma: a pitfall in aspiration cytology of the thyroid. Am J Clin Pathol. 2004 Apr;121(4):551-6. doi: 10.1309/NKED-4TJX-UENR-21M2. PMID: 15080307.
8. Sun ZQ, Guang HD, Ye JQ, Zhang W. Primary adenoid cystic carcinoma of thyroid gland: A case report. Asian J Surg. 2022 Feb;45(2):746-747. doi: 10.1016/j.asjsur.2021.11.041. Epub 2021 Dec 23. PMID: 34955347.
9. Duan X, Hu T, Cai H, Lin L, Zeng L, Wang H, Cao L, Li X. Radiotherapy for primary thyroid adenoid cystic carcinoma. Open Life Sci. 2023 Mar 7;18(1):20220547. doi: 10.1515/biol-2022-0547. PMID: 36910470; PMCID: PMC9993328
10. Baloch ZW, Segal JP, Livolsi VA. Unique growth pattern in papillary carcinoma of the thyroid gland mimicking adenoid cystic carcinoma. Endocr Pathol. 2011 Dec;22(4):200-5. doi: 10.1007/s12022-011-9174-7. PMID: 21863325.
11. Haji, Bahiyah E. et al. “Papillary thyroid carcinoma with an adenoid cystic pattern: Report of a case with fine?needle aspiration cytology and immunocytochemistry.” Diagnostic Cytopathology 30 (2004): n. Pag.
12. Ustün H, Atalay FO, Ekinci C. Adenoid cystic variant of papillary thyroid carcinoma: a case report with fine-needle aspiration cytology. Diagn Cytopathol. 2008 Jan;36(1):64-6. doi: 10.1002/dc.20716. PMID: 18064695
13. Malhotra, Purnima et al. “Poorly Differentiated Thyroid Carcinoma Mimicking Adenoid Cystic Carcinoma on Aspiration Cytology.” Acta Cytologica 53 (2009): 591 - 593.
14. Wan, Y., Long, C., Liu, Y. et al. Value of cytopathology in the diagnosis of adenoid cystic carcinoma and an analysis of misdiagnoses. BMC Surg 23, 52 (2023). https://doi.org/10.1186/s12893-023-01945-4
15. Tincani AJ, Del Negro A, Araújo PP, Akashi HK, Martins AS, Altemani AM, Barreto G. Management of salivary gland adenoid cystic carcinoma: institutional experience of a case series. Sao Paulo Med J. 2006 Jan 5;124(1):26-30. doi: 10.1590/s1516-31802006000100006. Epub 2006 Apr 3. PMID: 16612459
16. Miller, L.E.; Au, V.; Mokhtari, T.E.; Goss, D.; Faden, D.L.; Varvares, M.A. A Contemporary Review of Molecular Therapeutic Targets for Adenoid Cystic Carcinoma. Cancers 2022, 14, 992.