Physiological Interactions between the Cardiovascular and Endocrine Systems: Hyperthyroidism and Pulmonary Hypertension
Physiological Interactions between the Cardiovascular and Endocrine Systems: Hyperthyroidism and Pulmonary Hypertension
Avani Vinodbhai Mendpara*
Correspondence to: Avani Vinodbhai Mendpara, Consultant Physician (Internal Medicine), J Doshi Hospital, Rajkot (Gujarat), India.
Copyright
© 2024 Avani Vinodbhai Mendpara. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 10 Dec 2024
Published: 21 Dec 2024
Abstract:
Pulmonary hypertension is defined as the mean arterial pressure greater than 20 mmHg. Thyroid disorders may induce systemic manifestations of pulmonary hypertension (PH), physiological causes of which are not well understood. PH can be caused by a number of conditions, including HIV, connective tissue disorders, hypoxic chronic lung diseases, chronic thromboembolism, and left heart problems. Pulmonary hypertension secondary to Thyroid disorder is rare. Here we report a case of pulmonary hypertension caused by grave’s disease which emphasize the fact that physicians considering thyroid disorders causing pulmonary hypertension plays a pivotal role in reducing mortality and morbidity.
Physiological Interactions between the Cardiovascular and Endocrine Systems: Hyperthyroidism and Pulmonary Hypertension
Introduction
Pulmonary hypertension (PH) is defined as the mean pulmonary arterial pressure greater than 20 mmHg1; it requires a high degree of suspicion for diagnosis because of no specific signs and symptoms and low prevalence. Dyspnea on exertion, lower limb edema, hepatomegaly and syncope are commonly associated signs and symptoms of pulmonary hypertension2. Various conditions like left heart diseases, hypoxic chronic lung diseases, chronic thromboembolism, connective tissue diseases, hereditary diseases, HIV can cause PH1. Thyroid diseases causing pulmonary hypertension is a result of systemic manifestations of which the physiological mechanisms are unclear3.
Thyroid hormone effects the cardiovascular system due to 1) interactions with autonomic nervous system, 2) effect on vascular bed and endothelial function, 3) direct effect on cardiac tissues4. Hyper or Hypo thyroid levels exacerbate these effects. Thyroid hormone modulates the peripheral vascular tone by interfering in the biochemical cascade of the beta-adrenergic biochemical pathways. It has positive chronotropic and ionotropic effect on myocardial contraction.
Thyroid functional status influences the vascular tone by interfering with the alpha 1 adrenergic stimulation, it also alters the vascular wall morphology. Pulmonary vascular bed can be considered as a possible final target of these cardiac and vascular alterations. We present a case of Pulmonary hypertension caused by graves’ disease.
Case Details
A 57-year-old female presented to the hospital with chief complaints of breathlessness which was grade III MMRC since 1 week. Patient had no other significant clinical history. On examination patient’s vitals were stable and normal systemic examination. Routine blood investigations were normal.
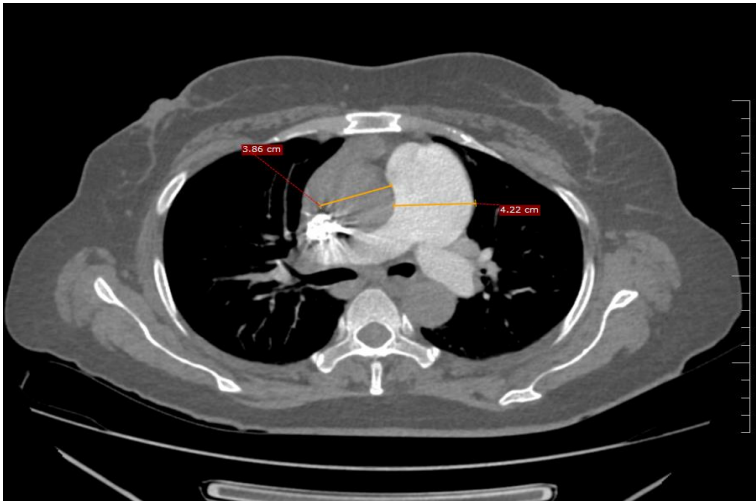
2D ECHO was done and it showed normal Left ventricle systolic function, ejection fraction 60%with moderate pulmonary hypertension (RVSP = 51mmhg). CT Thorax was done and it showed prominent main pulmonary artery and its branches with diffuse mosaic attenuation in bilateral lung fields, mild cardiomegaly and bilateral pleural effusion. Evaluation for pulmonary hypertension was done. D-dimer was 1.46 micro gram /ml. CT pulmonary angiogram was done and it showed no evidence of pulmonary thromboembolism. Anti-nuclear antibody (immunofluorescence) was negative. Thyroid profile was done and it showed TSH < 0.01 m IU/L free T3 11.6 pg/mL freeT4 4.7 ng/dL and anti-thyroid peroxidase >1000 IU/ml. Ultrasound of thyroid showed bilateral lobes of thyroid appearing bulky, heterogenous with increased with vascularity. Patient was diagnosed to have Grave’s disease and patient was started on oral carbimazole 5 mg twice a day.
Fig 1: Ct Chest Showing Dilated Main Pulmonary Artery With Reversal Of Aorta Pulmonary Ratio
Discussion
Pulmonary Hypertension is classified based on etiological and pathophysiological mechanisms into 5 groups. Group 1) idiopathic pulmonary artery hypertension, Group 2) because of left heart diseases, Group 3) due to hypoxia and chronic lung disease, Group 4) CTEPH, Group 5) due to unknown mechanisms5. The possibilities of group 2, group3, group 4 in this case were ruled out with normal CTPA, normal left ventricular function and no prior history of lung conditions hypoxia. Due to hyperthyroidism in our patient, we classified it as group 5 which is associated with metabolic disorders.
Majority of the hyperthyroid cases up to 80% are due to graves’ disease. The cardiovascular effect of thyrotoxicosis has been well documented in many studies. The association between PH and hyperthyroidism can be either etiological or incidental. No clear pathogenetic mechanisms have been described. Few hypotheses have been proposed of which the main one is the autoimmune hypothesis6. It describes the possible indirect influence of thyroid stimulating hormone receptor antibodies in inducing an immune mediated damage of the vascular endothelium which promotes endothelial dysfunction and develops PH. All patients with graves’ disease do not develop PH so few other mechanisms also have been described which are not in the scope of our discussion.
Few studies describing the prevalence of hyperthyroidism and pulmonary hypertension are SUE et al described 47% of pulmonary hypertension in the study population of 75 patients with hyperthyroidism7. Marvisi et al reported 35% mild PH in patients suffering with grave’s disease and multinodular goiter8. A study by Trapp et al found that the combination of PH hyperthyroidism might induce acute cardiopulmonary decompensation decreasing the patient’s survival, this also signifies the importance of aggressive treatment of hyperthyroidism either pharmacologically or surgically to improve patient’s survival9. Hypothroidism also causes pulmonary hypertension and the prevalence have been reported at 24% in few studies10.
There are no prospective studies for the treatment of PH due to hyperthyroidism. Few studies and case reports showed significant reduction in pulmonary artery pressure with thyroid suppression drugs suggesting their role in improving the hemodynamic status of patients11.Our case responded well to anti thyroid suppression drugs and clinal symptoms came down.
Conclusion
Pulmonary hypertension group 5 needs extensive evaluation due to its wide range of etiological factors and so rong suspicion is needed. As both hyper and hypo thyroid levels are known to cause pulmonary hypertension a routine thyroid investigation is a mandatory part of pulmonary hypertension evaluation
References
1. Simonneau G, Montani D, Celermajer DS, Denton CP, Gatzoulis MA, Krowka M, et al. Haemodynamic Definitions and Updated Clinical Classification of Pulmonary Hypertension. Eur Respir J (2018) 53 (1):1801913. doi: 10.1183/13993003.01913-2018
2: Domenighetti G. Prognosis, Screening, Early Detection and Differentiation of Arterial Pulmonary Hypertension. Swiss Med Wkly (2007) 137(23–24):331–6.
3: Scicchitano P, Dentamaro I, Tunzi F, Ricci G, Carbonara S, Devito F, et al. Pulmonary Hypertension in Thyroid Diseases. Endocrine (2016) 54(3):578– 87. doi: 10.1007/s12020-016-0923-8
4: H. Vargas-Uricoechea, A. Bonelo-Perdomo, C.H. Sierra-Torres, Effects of thyroid hormones on the heart. Clin. Investig. Arterioscler. 26, 296–309 (2014)
5: Guidelines for the treatment of pulmonary hypertension (JCS 2017/JPCPHS 2017) Fukuda K, Date H, Doi S, et al. Circ J. 2019;83:842–945.
6: T. Sugiura, S. Yamanaka, H. Takeuchi, N. Morimoto, M. Kamioka, Y. Matsumura, Autoimmunity and pulmonary hypertension in patients with Graves’ disease. Heart Vessel. 30, 642–646 (2015)
7: C.W. Siu, X.H. Zhang, C. Yung, A.W. Kung, C.P. Lau, H.F. Tse, Hemodynamic changes in hyperthyroidism-related pulmonary hypertension: a prospective echocardiographic study. J. Clin. Endocrinol. Metab. 92, 1736–1742 (2007)
8: M. Marvisi, P. Zambrelli, M. Brianti, G. Civardi, R. Lampugnani, R. Delsignore, Pulmonary hypertension is frequent in hyperthyroidism and normalizes after therapy. Eur. J. Intern. Med. 17, 267–271 (2006)
9: C.M. Trapp, R.W. Elder, A.T. Gerken, A.B. Sopher, S. Lerner, G.S. Aranoff, E.B. Rosenzweig, Pediatric pulmonary arterial hypertension and hyperthyroidism: a potentially fatal combination. J. Clin. Endocrinol. Metab. 97, 2217–2222 (2012)
10. A.L. Curnock, R.A. Dweik, B.H. Higgins, H.F. Saadi, A.C. Arroliga, High prevalence of hypothyroidism in patients with primary pulmonary hypertension. Am. J. Med. Sci. 318, 289–292 (1999)
11. R. Thurnheer, R. Jenni, E.W. Russi, P. Greminger, R. Speich, Hyperthyroidism and pulmonary hypertension. J. Intern. Med. 242, 185–188 (1997).