Unusual Incidental Finding of Primary Bone Leiomyosarcoma
Unusual Incidental Finding of Primary Bone Leiomyosarcoma
Mohammed Abdelmohsin Khairelseed*1,Bader Said Almarboiee*2,Wail Moahmoud*3,Ahmed Khairy*4
1, 3, 4. -Orthopedic department Buraimi Hospital, Oman.
2-Orthopedic department Buraim Hospital HOD, Oman.
*Correspondence to: Mohammed Abdelmohsin Khairelseed, Buraimi Hospital, Oman.
Copyright
© 2024 Mohammed Abdelmohsin Khairelseed This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 30 Nov 2024
Published: 24 Dec 2024
Abstract:
We present a 33 years old Omani lady with Primary bone leiomyosarcoma of distal tibia which had been diagnosed after she sustained a subtle ankle injury, the radiograph showed 2.5 cm osteolytic lesion, biopsy documents the presence of undifferentiated spindle cells neoplasm, with the presence of smooth muscle actin SMA, desmin and vimentin in immunohistochemistry suggesting a low grade bone leiomyosarcoma, although distant metastases quit common in high grade tumors as reported by authors ,the course of the disease was rapid in our patient with occurrence of lung and pelvic metastasis 7 month after being diagnosed , neoadjuvant chemotherapy seems to be ineffective in preventing distant metastasis.
Unusual Incidental Finding of Primary Bone Leiomyosarcoma
Introduction
According to American bone cancer statistics 2023, Primary Bone cancers represent 1 % of body malignancies, with annual incidence of 0.9 % per 100,000 population .(1) Primary bone leiomyosarcoma represents only 0.7 % of this percentage. it is characterized by the smooth muscles differentiation and absence of osteoid matrix. Leiomyosarcoma is seen frequently more in soft tissues of retroperitoneum and genitourinary tract. (2)
Thae First case that had been reported by Evans and Sanerkin in 1965, the reported median age is 45 years with wide range of presentation 9-88 years, equal gender distribution with slight female predominance (3) . it can affect various bones but most frequently seen in long bones mostly distal femur and proximal tibia, fascial and cranial bone are also involved in 20% of cases. (4)
The usual presenting feature of primary bone leiomyosarcoma is mild to moderate pain, swelling with or without pain and pathological fractures also can be a presenting feature. (5) presence of metaphyseal intramedullary osteolytic lesion, cortical destruction and periosteal reaction is the most common radiological findings, adjacent soft tissue involvement is seen in advanced cases, Kameda et al reviewed 30 case of primary bone leiomyosarcoma, osteolytic bone lesion was seen in 90 % of cases , the mean and average diameter 7 cm .(7)
The unique characteristic histopathological findings that differentiate primary bone leiomyosarcoma from other fibroblastic and histiocytic cell tumors is the presence of heterogenous groups of spindle cells with rod-shaped or cigar-shaped hyperchromatic nuclei together the presence of smooth muscles actin and desmin in immunohistochemistry test which in most primary bone
leiomyosarcoma. The absence of chondroid and osteoid matrices differentiates leiomyosarcoma from the most common bone sarcomas osteosarcoma and chondrosarcoma. (8)
The course of primary bone leiomyosarcoma is usually aggressive, the histological grade and clinicopathological grade are the most important predictors of prognosis , high grade tumors has a high probability for local recurrence and distal metastasis. (6) due to paucity of clinical date other prognostic factors which determines the severity of the disease still not well documented in literature , however the 5 years survival rate of primary bone leiomyosarcoma ranges from 62-up to 78 percentage .Brewer et al studied 33 patients with Primary bone leiomyosarcoma, they reported an overall 5 years survival rate of 62% at five years , patients with stage 1 or 2a had 100% survival rate , patients with stage 2b tumors had a 60% survival at 5 years, and patients with stage 3 tumors had a median survival of 2 years, but all had died within four years. (9)
Metastasis tends to occur at the first year of diagnosis mainly involving lungs ,liver and axial skeleton, metastasis is more frequently seen in high grade lesions , it carries poor prognosis. (10) The main option of cure of primary bone leiomyosarcoma is surgical resection with negative surgical margins before the presence metastasis. In a case series that had studied 31 patients with primary bone leiomyosarcoma ,28 patients have been treated surgically 8 patient was treated with amputation and 20 with limb salvage , three patients had a local recurrence but half of patients had developed distant metastasis All patient disease-specific survival was 57% at five years but for those without metastases was 82%. (9)
No data till now proves the effectiveness of chemotherapy or radiotherapy as adjuvant or neoadjuvant therapy in surgical cure or downgrading of primary bone leiomyosarcoma, they also been used as palliative settings but their role is not will confirmed due to lack of level I evidences in literature. A case series 48 patients of primary bone leiomyosarcoma 18 patients had been treated with neoadjuvant chemotherapy the regimen (cisplatin-based chemotherapy) was used, none of the patients shown a good response by histological or radiological assessment. (11)
Case Report Description
Clinical features:
A 33 years old lady who have no previous history of chronic illness, attended to emergency department in May 2022 after she twisted her left ankle on same day, complaining of left ankle pain, there was no ankle swelling but there was a limitation of ankle movements, radiograph of her left ankle was initially overlooked, analgesia and splint was provided and patient was given appointment to orthopedic clinic.
Investigations:
Patient was evaluated in our clinic, the radiograph showed the presence of distal tibial metaphyseal rarefaction and osteolytic lesion of about 2.5* 2.5 cm, there was no periosteal reaction or destruction and no soft tissue involvement (figure1). Blood parameters, bone profile and inflammatory markers were with in normal.
Figure 1: a radiograph of distal tibia showing an intramedullary osteolytic lesion 5-7 cm from tibiotalar articular magin with surrounding rarefaction with no obvious cortical distruction
MR
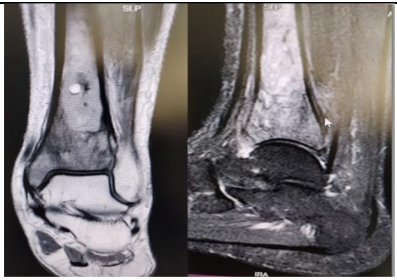
MR imaging showed the presence of distal tibial 3*2*1 cm partially defined cyst, with a narrow zone of transition with heterogenous enhancement in the surrounding bone marrow, cortical thinning and smooth periosteal elevation, suggesting a neoplastic etiology , no soft tissue or vascular involvement or skip lesions (figure2).
Figure 2: Magnetic resonance imaging of left distal tibia showing distal tibial osteolytic lesion with narrow zone of transition with surrounding medullar altered signal intensities with heterogenous contrast, periosteal elevation and thinning suggesting a neoplasm.
Patient was evaluated by Multidisciplinary team ,needle biopsy of the lesion showed presence of malignant undifferentiated spindle cell neoplasm in favor of Fibroblastic Osteosarcoma however Undifferentiated Sarcoma was not ruled out.
Diagnosis
Open biopsy of the lesion was double confirmed by presence of primary bone leiomyosarcoma in a highly specialized center by the presence of heterogeneous smooth muscles with presence of desmin and smooth muscle actin, tumor cells diffusely positive for vimentin, scattered MDM-2,P53 nuclear staining, tumor cells are negative for LCA,Pax-5,CD20-CD30-ALK.
Initial CT scans and PET scans of whole body were normal.
Treatment and follow up
A multidisciplinary team approach was initiated, oncology center suggested a limited value of neoadjuvant chemotherapy and the patient was given the opportunity to choose between a limb salvage surgery with the use of vascularized fibula graft with wide local excision together with arthrodesis of ankle joint and the other option is amputation with use of external prosthesis, the use of distal tibia endoprosthesis with it is risks and possible complications had also been explained.
The patient choose to seek another opinion from another center and advised neoadjuvant chemotherapy followed by surgery and radiotherapy, started neoadjuvant chemotherapy four cycles with IFOS+IDR on December 2022 with poor patient tolerance.
Outcome
During these sessions the patient was presented with chest pain, CT scan showed presence of basal lung metastasis and PET scan also showed presence of pelvic bone metastasis. Patient seeks advice from another center, limb amputation was carried out, patient is still under follow up there.
Discussion
Primary bone leiomyosarcoma is a rare disease, represents 0.7% of primary bone sarcomas, the mean age of occurrence is 45 years. (3) Male to female ratio is equal with slight female predominance which may be attributed to hormonal influences as suggested by some authors. (2)(6) In our case the patient was suffering from infertility, and she was seeking management for this issue which may have clinical correlation. The most common disease presentation is pain and swelling and pathological fractures. (5) Although in our case incidental discovery was the predominant, going into retrograde inquiry the patient was complaining of low-grade pain in left ankle for a few months before the presentation.
The presence of undifferentiated spindle cells in microscopy and smooth muscle actin and desmin in immunohistochemistry is a characteristic finding that differentiates primary bone leiomyosarcoma from other fibro sarcomatous bone tumors. (12) Metastatic leiomyosarcoma was ruled out by absence of primary lesions in the gastrointestinal, genitourinary tracts and retroperitoneum, presence of osteogenesis is a characteristic for fibrous osteosarcoma which as absent is this case. Expression of p63 and PAX8 together with absence of myogenic tumor markers such as smooth muscle actin and desmin represents the characteristic features in metastatic sarcomatous carcinomas. (12)
Metastasis usually occurs in the first year of disease presentation, the cause of this is still uncertain. (2) our case can serve as a reference for this since metastasis was documented after 7 months of initial presentation. Usually, metastasis occurs in histological high-grade lesions. (6) In our case, even though low-grade lesion was confirmed metastasis did occur, there is a probability that the cause of this is a delay in management initiation since the patient’s decision to start the management was relatively late.
Early and effective radical surgery with a negative surgical margin represents the corner stone in disease cure and best prognosis, The use of chemotherapy as adjuvant and new adjuvant regimen is a matter of discussion, there effectiveness needs to be investigated with more future studies, our case can serve as a reference of ineffectiveness of neoadjuvant chemotherapy in preventing disease progression in form of distant metastasis. Jundt et al published a case series of 8 patient who had been treated with neoadjuvant and adjuvant chemotherapy with poor outcome and occurrence of distant metastasis during follow up. (13) Antonescu et al conducted a retrospective study on 33 patients with primary bone leiomyosarcoma, 21% of them received adjuvant and neoadjuvant chemotherapeutic regimens with no survival differences, he also reported ineffectiveness of radiotherapy in improvement of the outcome of the cases. (6)
Conclusion
Primary bone leiomyosarcoma is a rare but aggressive type of bone sarcomas, early detection and rapid radical surgery is the main pillar for cure, the role of adjuvant and neoadjuvant chemotherapy need to be further investigated and further researches are needed to identify disease prognostic factors
References
1-Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. Ca Cancer J Clin. 2023 Jan 1;73(1):17-48.
2-Zumárraga JP, Arouca MM, Baptista AM, Caiero MT, Rubio DE, Camargo OP. Primary leiomyosarcoma of bone: clinicopathologic and prognostic factors analysis in a single institution. Acta ortopedica brasileira. 2019 May 30;27:152-5.
3-Zumárraga JP, Arouca MM, Baptista AM, Caiero MT, Rubio DE, Camargo OP. Primary leiomyosarcoma of bone: clinicopathologic and prognostic factors analysis in a single institution. Acta ortopedica brasileira. 2019 May 30;27:152-5.
4-Brewer P, Sumathi V, Grimer RJ, Carter SR, Tillman RM, Abudu A, Jeys L. Primary leiomyosarcoma of bone: analysis of prognosis. Sarcoma. 2012 Jan 1;2012.
5-Rekhi B, Kaur A, Puri A, Desai S, Jambhekar NA. Primary leiomyosarcoma of bone—a clinicopathologic study of 8 uncommon cases with immunohistochemical analysis and clinical outcomes. Annals of Diagnostic Pathology. 2011 Jun 1;15(3):147-56.
6- Antonescu CR, Erlandson RA, Huvos AG. Primary leiomyosarcoma of bone: a clinicopathologic, immunohistochemical, and ultrastructural study of 33 patients and a literature review. The American journal of surgical pathology. 1997 Nov 1;21(11):1281-94.
7-Kameda N, Kagesawa M, Hiruta N, Akima M, Ohki M, Matsumoto T. Primary leiomyosarcoma of bone: a case report and review of the literature. Pathology International. 1987 Feb;37(2):291-303.
8-Wu Z, Cheng L, Cao Q, Ye S, Yu S, Sun M, Jing J. Case report and literature review: Primary leiomyosarcoma of the bone in the trochanteric region of the femur. Frontiers in Surgery. 2023 Jan 10;9:1045307.
9-Brewer P, Sumathi V, Grimer RJ, Carter SR, Tillman RM, Abudu A, Jeys L. Primary leiomyosarcoma of bone: analysis of prognosis. Sarcoma. 2012 Jan 1;2012.
10-Recine F, Bongiovanni A, Casadei R, Pieri F, Riva N, De Vita A, Mercatali L, Liverani C, Spadazzi C, Miserocchi G, Fausti V. Primary leiomyosarcoma of the bone: a case report and a review of the literature. Medicine. 2017 Nov;96(45).
11- Mori T, Nakayama R, Endo M, Hiraga H, Tomita M, Fukase N, Kobayashi E, Kawai A, Ueda T, Morioka H. Forty?eight cases of leiomyosarcoma of bone in Japan: a multicenter study from the Japanese musculoskeletal oncology group. Journal of Surgical Oncology. 2016 Sep;114(4):495-500.
12- Wu Z, Cheng L, Cao Q, Ye S, Yu S, Sun M, Jing J. Case report and literature review: Primary leiomyosarcoma of the bone in the trochanteric region of the femur. Frontiers in Surgery. 2023 Jan 10;9:1045307.
13- Jundt G, Moll C, Nidecker A, Schilt R, Remagen W. Primary leiomyosarcoma of bone: report of eight cases. Human pathology. 1994 Nov 1;25(11):1205-12.