Incidence and Risk Factors of Myocardial Infarction in Patients Presented with Ischemic Stroke.
Incidence and Risk Factors of Myocardial Infarction in Patients Presented with Ischemic Stroke.
Abdullah Fahad Alghamdi1, Ghada Merdad2, Alhassin Ghazy S Alsulymani *3, Raed Ateeq M Alsulami4, Hassan Ahmed Hazazi5, Ali Salem Al- Dawais6, Abdulrahman Aidah Al ghashmari7, Asim Mussad Almalawi8, Muhannad Mohammed A Algarni9
1. ER Resident, king Abdullah complex hospital, Jeddah, Saudi Arabia.
2. ER consultant, king abdulaziz university hospital, Jeddah, Saudi Arabia.
4. IM Resident, East Jeddah General hospital, Jeddah, Saudi Arabia.
5. GP, King Fasial Hospital, Al-Taif.
6,7,9. Medical student, king abdulaziz university hospital, Jeddah, Saudi Arabia
8. Neurology Resident, Dr.Soliman Fakeeh Hospital, Jeddah, Saudi Arabia.
*Correspondence to: Alhassin Ghazy S Alsulymani, IM Resident, King Fahad General Hospital, Jeddah, Saudi Arabia.
Copyright
© 2024 Alhassin Ghazy S Alsulymani. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 17 Dec 2024
Published: 02 Jan 2025
Abstract
Background: Myocardial infarction (MI) and ischemic stroke (IS) represent simultaneous medical emergencies requiring immediate attention. Myocardial infarction (MI) refers to any event that leads to reduced blood flow to the heart muscle, causing cardiac cell death. In contrast, ischemic stroke (IS) denotes the abrupt onset of inadequate blood supply to a specific brain region, resulting in a decline in neurological function. The factors that increase the likelihood of experiencing ischemic stroke or myocardial infarction overlap, as do the physiological mechanisms driving these conditions. Studies regarding the occurrence and connection between heart attacks and strokes in the Middle East are limited. Therefore, the aim of this study was to determine the incidence and risk factors of myocardial infarction in patients presenting with ischemic stroke.
Method: In this retrospective cohort study conducted at King Abdul-Aziz University Hospital in Jeddah, Saudi Arabia, during June 2023, we analyzed 27 out of 1,176 stroke patients at KAUH from 2017 to 2022 who subsequently experienced a heart attack (MI) during the study period.
Results: The study revealed an incidence rate of 14% per patient-year for MI following ischemic stroke, with a substantial occurrence within the first year. ST-Elevation Myocardial Infarction (STEMI) was predominant (51.9%) post-stroke. Patients with comorbidities such as Peripheral Arterial Disease (PAD), heart failure, and a history of smoking exhibited a higher likelihood of earlier onset MI after stroke. However, age, gender, BMI, family history of MI, hypertension, diabetes, and atrial fibrillation did not significantly influence the duration between stroke and MI.
Conclusion: The study found a 14% yearly rate of heart attacks in patients with ischemic stroke, with most occurring within the first year; however, a significant number experienced it beyond the initial year. Peripheral Arterial Disease, heart failure, and smoking were key risk factors. These results highlight the need for targeted interventions and new screening guidelines to detect and prevent heart attacks early in this population.
Incidence and Risk Factors of Myocardial Infarction in Patients Presented with Ischemic Stroke.
Introduction
Myocardial infarction (MI) and ischemic stroke (IS) are medical emergencies that require urgent medical attention. (1) Myocardial infarction (MI) is defined as any incident that causes myocardial ischemia, resulting in cardiac myocyte cell death, while ischemic stroke (IS) is defined as the sudden occurrence of acute ischemia in a specific area of the brain, resulting in loss of neurological function. (2, 3) The risk factors for ischemic stroke and myocardial infarction are similar, as is the pathophysiological process. (4) Worldwide, ischemic stroke is the second leading cause of death and a significant contributor to disability. (5, 6) According to the WHO, the two main causes of death worldwide, stroke and ischemic heart disease (IHD), accounted for approximately 8.76 million and 6.24 million deaths in 2015, respectively. (7) There is evidence that patients who have had an ischemic stroke are at significant risk of developing coronary artery disease (CAD). (8) A previous systematic review has established that the incidence of MI after ischemic stroke is 1.67% and 2%. (4, 8) Furthermore, a cohort study in 2022 with a 5-year follow-up showed an incidence of 11.1%. (7) A study conducted in Korea on recurrent stroke, myocardial infarction, and major vascular events during the first year showed a cumulative incidence at 30-day, 90-day, and 1-year rates of 1%, 3%, and 5%, respectively, for MI after ischemic stroke. (9) There are common risk factors that contribute to the pathophysiology of MI and IS, such as age, smoking, male gender, diabetes mellitus (DM), hypertension (HTN), peripheral artery disease (PAD), coronary artery disease (CAD), and chronic kidney disease (CKD). (8-12) It is still controversial whether stroke patients should be screened for asymptomatic coronary artery disease. (4) Studies regarding the incidence and relationship between myocardial infarction and ischemic stroke in the Middle East are limited. Hence, the purpose of this study was to determine the incidence and risk factors of myocardial infarction in patients presenting with ischemic stroke at King Abdulaziz University Hospital (KAUH), Jeddah, Saudi Arabia.
Materials & Methods
Aim and Objectives
This study aimed to determine the incidence and risk factors of myocardial infarction in patients presenting with ischemic stroke from 2017 to 2022 at King Abdul-Aziz University Hospital (KAUH) in Jeddah, Saudi Arabia.
Study Design and Settings
This retrospective cohort study was conducted in June 2023 at King Abdul-Aziz University Hospital (KAUH), a tertiary care center in Jeddah, Saudi Arabia. The study involved all patients presenting at the emergency department with ischemic stroke from 2017 to 2022. The study was approved by the KAUH Ethical Committee, reference number (285-23).
Study Population and Sample Size
We reviewed the medical records of 1,176 patients who presented with stroke from 2017 to 2022 at KAUH. Twenty-seven of them met the inclusion criteria, which included any patient with ischemic stroke during that period who subsequently presented with myocardial infarction (MI). Patients with hemorrhagic stroke, transient ischemic attack (TIA), or a previous history of MI prior to the ischemic stroke were excluded.
Data Collection and Definition of Variables
Data were obtained from the Hospital Health Informatics Department, collected, and interpreted using a data collection sheet and Microsoft Excel. The collection sheet contained demographics, including patient age, gender, and body mass index.
The date and type of MI were recorded, as well as the date of ischemic stroke diagnosis and the use of percutaneous coronary intervention (PCI).
The risk factors assessed in the study included a family history of MI, smoking history, diagnosis of heart failure, diabetes, hypertension (HTN), peripheral artery disease (PAD), and atrial fibrillation.
Medication history was also collected, including antiplatelet agents, anticoagulants, statins, antihypertensive medications, diabetic medications, and thrombolytic medications.
Laboratory investigations measured included troponin, creatine kinase-MB (CK-MB), total cholesterol, low-density lipoprotein (LDL), high-density lipoprotein (HDL), triglycerides, and hemoglobin A1c (HbA1c) levels.
Data Entry and Data Analysis
Data were analyzed using the Statistical Package for Social Sciences (SPSS) (IBM SPSS, IBM Corp., Armonk, N.Y., USA) version 26. Univariate analysis was conducted to assess the frequency of categorical variables and the central tendency and measures of dispersion for continuous variables. The Chi-squared test (χ2) was applied to investigate the association between qualitative variables, expressed as numbers and percentages. The Mann–Whitney U and Kruskal-Wallis tests were used to examine the association between nonparametric quantitative variables, expressed as means and standard deviations (mean ± S.D.). Statistical significance was defined as p < 0.05.
Result
In this study, 27 patients were included out of 1176 (2.23%) with incidence rate of about 14 per 100 patient each year. The patient age ranged from 39 to 87 years with mean age was 65.56 ± 13.48 years and BMI ranged from 17.30 to 49.54 (kg/m2) with mean 30.49±7.19 (kg/m2). The males were more than females (63% versus 37%). Most of the cases had a ST Elevation Myocardial infarction (STEMI) (51.9%) followed by Unstable Angina (UA) (22.2%) and Non-ST Elevation Myocardial Infarction (NSTEMI) (14.8%). Of patients 33.3% were smokers, 25.9% had positive family history of MI. Associated comorbidities were 92.9% hypertensive, 70.4% diabetics, 40.7% heart failure, 18.5% atrial fibrillation and 11.1% peripheral arterial diseases. Medications used were Statin (100.0%), antihypertensive (96.3%), antiplatelet (77.8%), anticoagulants (70.4%), diabetic medications (66.7%), PCI (25.9%) and thrombolytic medications (22.2%) (Table 1).
Table 1. Demographic and clinical characteristics of patients (N=27).
|
Characteristics |
Count |
% |
|
|
Age (years) |
Mean ± SD |
65.56 ± 13.48 |
|
|
BMI (kg/m2) |
Mean ± SD |
30.49±7.19 |
|
|
Gender |
Male |
17 |
63.0% |
|
Female |
10 |
37.0% |
|
|
Type of MI |
STEMI |
14 |
51.9% |
|
UA |
6 |
22.2% |
|
|
NSTEMI |
4 |
14.8% |
|
|
Unspecified MI |
3 |
11.1% |
|
|
Risk factors |
|
|
|
|
Smoker |
Yes |
9 |
33.3% |
|
Family History of MI |
Yes |
7 |
25.9% |
|
Comorbidities |
|
|
|
|
Hypertension |
Yes |
25 |
92.6% |
|
Diabetes Mellitus |
Yes |
19 |
70.4% |
|
Heart Failure |
Yes |
11 |
40.7% |
|
Atrial Fibrillation |
Yes |
5 |
18.5% |
|
Peripheral Arterial Disease |
Yes |
3 |
11.1% |
|
Medications used |
|
|
|
|
Statin |
Yes |
27 |
100.0% |
|
Antihypertensive |
Yes |
26 |
96.3% |
|
Antiplatelet |
Yes |
21 |
77.8% |
|
Anticoagulant |
Yes |
19 |
70.4% |
|
Diabetic Medications |
Yes |
18 |
66.7% |
|
PCI |
Yes |
7 |
25.9% |
|
Thrombolytic |
Yes |
6 |
22.2% |
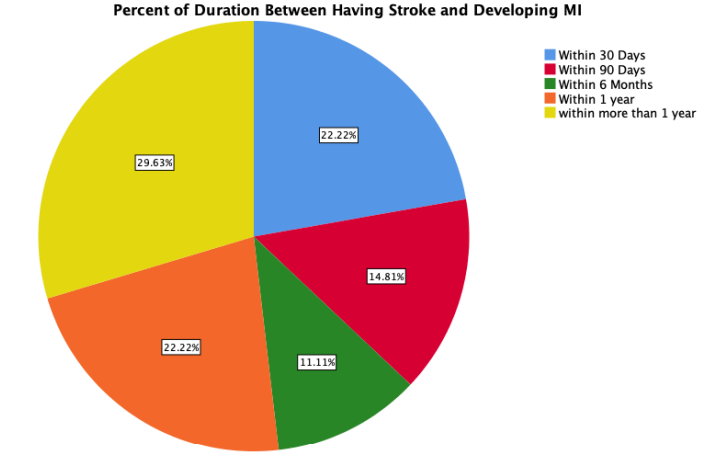
Figure 1: Percentage of duration between having a stroke and developing MI.
The duration of having MI after stroke was significantly more within 30 days in patients with heart failure (P =0.020) and peripheral artery diseases (P = 0.021). Meanwhile, in smokers, the duration of having MI after stroke was significantly more > 1year (P = 0.021). There were insignificant differences in the duration of having MI after stroke in patients with a positive family history of MI, Diabetes Mellitus, Atrial Fibrillation, hypertension as well as age and BMI (P= 0.067, P= 0.732, P= 0.759, P= 0.274, P= 0.956, and p= 0.876, respectively) (Table 2).
Table 2 - The Relationship Between the Duration before MI and Risk factors.
|
Risk factors |
Duration of having MI after stroke |
Significance |
||||||||||
|
|
30 Days |
90 Days |
6 Months |
1 year |
> 1 year |
|
||||||
|
N |
% |
N |
% |
N |
% |
N |
% |
N |
% |
P-Value |
||
|
Heart Failure |
Yes |
5 |
45.5% |
1 |
9.1% |
1 |
9.1% |
3 |
27.3% |
1 |
9.1% |
0.020* |
|
No |
1 |
6.3% |
3 |
18.8% |
2 |
12.5% |
3 |
18.8% |
7 |
43.8% |
|
|
|
Peripheral Arterial Disease |
Yes |
3 |
100.0% |
|
|
|
|
|
|
|
|
0.021* |
|
No |
3 |
12.5% |
4 |
16.7% |
3 |
12.5% |
6 |
25.0% |
8 |
33.3% |
|
|
|
Smoker |
Yes |
2 |
22.2% |
|
|
|
|
3 |
33.3% |
4 |
44.4% |
0.026* |
|
No |
4 |
22.2% |
4 |
22.2% |
3 |
16.7% |
3 |
16.7% |
4 |
22.2% |
|
|
|
Family History of MI |
Yes |
2 |
28.6% |
|
|
2 |
28.6% |
3 |
42.9% |
|
|
0.067 |
|
No |
4 |
20.0% |
4 |
20.0% |
1 |
5.0% |
3 |
15.0% |
8 |
40.0% |
|
|
|
Diabetes Mellitus |
Yes |
5 |
26.3% |
2 |
10.5% |
2 |
10.5% |
5 |
26.3% |
5 |
26.3% |
0.732 |
|
No |
1 |
12.5% |
2 |
25.0% |
1 |
12.5% |
1 |
12.5% |
3 |
37.5% |
|
|
|
Atrial Fibrillation |
Yes |
2 |
40.0% |
1 |
20.0% |
|
|
1 |
20.0% |
1 |
20.0% |
0.759 |
|
No |
4 |
18.2% |
3 |
13.6% |
3 |
13.6% |
5 |
22.7% |
7 |
31.8% |
|
|
|
Hypertension |
Yes |
6 |
24.0% |
4 |
16.0% |
3 |
12.0% |
6 |
24.0% |
6 |
24.0% |
0.274 |
|
No |
|
|
|
|
|
|
|
|
2 |
100.0% |
|
|
|
Age (years) |
|
|
65±15 |
|
65±14 |
|
66±24 |
|
68±10 |
|
64±14 |
0.956 |
|
BMI (kg/m2) |
|
|
29.73± 7.73 |
|
33.07± 9.00 |
|
26.78± 8.50 |
|
31.41± 9.28 |
|
30.48 ± 4.66 |
0.876 |
Regarding the medication of use, there was no significant correlation between the risk of MI following stroke with the use of anticoagulant, antiplatelet, DM or HTN medication, Thrombolytic use for the stroke (p=0.274, p=0.749, p=0.859, p=0.201, p=0.661, respectively) (Table 3).
Discussion
In our study, we found that the incidence rate was 14 per 100. This finding is consistent with that of Buckley BJR et al., who found an incidence of 11.1%. [5] On the other hand, Pana TA et al., Kang K et al., and Alqahtani F et al. found lower rates. [7, 9, 10] Therefore, the differences between these studies are likely the result of various factors, such as differences in study design, sample size, and demographic characteristics. We believe our population has a longer survival rate due to a younger age; hence, they can develop subsequent MI.
Our statistical analysis indicates that the majority of patients develop myocardial infarction within the first year after being diagnosed with ischemic stroke. This can be attributed to underlying pathophysiology, shared risk factors, challenges in prevention, and the inflammatory response triggered by stroke [4, 8-12]. Understanding these relationships is critical for healthcare practitioners to create effective strategies for managing and preventing cardiovascular complications among individuals with ischemic stroke.
Interestingly, our research demonstrates that patients with Peripheral Arterial Disease (PAD) or heart failure are more likely to have MI within a year or less of experiencing an ischemic stroke. Conversely, another study shows that individuals with PAD or heart failure are prone to developing MI 1–5 years following a stroke. [7] This can be attributed to poorly controlled cardiovascular comorbidities, such as heart failure or PAD, within the first year following an ischemic stroke and ongoing disease processes, such as inflammation and atherosclerosis, provoked by stroke events [13]. To lower the risk of post-ischemic stroke MI, we recommend focusing on surveillance and improving the standard of care for patients with a history of cardiovascular comorbidities who present with ischemic stroke.
This study found that smoking significantly increases the likelihood of myocardial infarction (MI) following a stroke. The presence of smoking as a risk factor amplifies the vulnerability of stroke survivors to the development of MI, potentially due to synergistic effects on vascular damage and systemic inflammation. Further investigation into the mechanisms underlying this association may elucidate pathways for targeted interventions aimed at reducing the risk of MI in post-stroke individuals, particularly those with a history of smoking. [14, 15, 16]
Nonetheless, the current investigation finds that age, male gender, BMI, having a family history of MI, and having a diagnosis of hypertension (HTN), diabetes mellitus (DM), or atrial fibrillation (Afib) are not correlated with the duration between ischemic stroke and MI. These findings are consistent with those of Kang K et al., except for one finding that shows a significant risk of developing MI after a stroke with increasing age. [9] Since most of the patients in this study experienced MI in the first year following a stroke, we can infer that the majority of these parameters are chronic and require a longer duration to impact the interval between ischemic stroke and the development of MI. [17]
In our study, we found no significant correlation between the risk of MI following a stroke and the use of anticoagulants, antiplatelets, DM or HTN medications, thrombolytic use for the stroke, HbA1c, total cholesterol level, LDL and HDL levels, and cardiac enzymes, including CK-MB and troponin levels. This finding is consistent with some previous studies but not all. For example, a study by Fahad Alqahtani et al. found that thrombolytic use was significantly associated with a decreased risk of MI following stroke. [10] Another study by Long Li et al. found that early antiplatelet therapy within 48 hours at discharge decreased the associated risk of MI following stroke; however, they found that the use of antihypertensive medication was insignificant. [12] Additionally, Jaymala Mishra et al. found in their study that cardiac markers (CK-MB and troponin) had no role in the increased incidence of MI following a stroke in all age groups. [1] Another study supported our results, finding that cholesterol levels at the time of admission for MI after stroke were insignificant. [7] Lastly, a study by Thomas Mooe et al. supports our finding that anticoagulant and thrombolytic therapy were insignificant with regard to MI following stroke. [11]
It is important to note that these studies were all observational studies, which means that they cannot prove cause and effect. Overall, the evidence on the relationship between medication use, lab results, and the risk of MI after stroke is inconclusive. More research is needed to confirm these findings and clarify the role of these medications in preventing MI after stroke.
Limitations
Even though this study has provided valuable insights, it is not without limitations. The use of a retrospective design based on medical records may have led to potential gaps or errors in the data. Moreover, the study's focus on a single health facility highlights the need to be careful when extending the findings to larger populations. These limits emphasize why we need more studies in various healthcare setups. It'll help us truly grasp all the different aspects of the relationship between Myocardial infarction and Stroke.
Conclusion
This study sought to assess the incidence and risk factors of myocardial infarction (MI) in patients presenting with ischemic stroke. Our findings revealed a 14% patient-year incidence rate, with most cases occurring within the first year. Peripheral arterial disease, heart failure, and smoking emerged as prominent risk factors for MI development after ischemic stroke.
The implications of these results are substantial. They offer valuable insights for tailoring interventions aimed at high-risk patient groups, potentially shaping new screening and diagnostic guidelines for the early identification, treatment, and prevention of MI within this specific patient population.
Reference
1. Mishra J, Kumar A, Kumar S, Singh S, Kumar Nayan S, Dev A. Incidence of Acute Myocardial Infarction in Patients Presenting With Cerebrovascular Accident in a Tertiary Care Centre in Eastern India. Cureus. 2022;14(9):e29005.
2. Thygesen K, Alpert JS, White HD, Joint ESCAAHAWHFTFftRoMI, Jaffe AS, Apple FS, et al. Universal definition of myocardial infarction. Circulation. 2007;116(22):2634-53.
3. Phipps MS, Cronin CA. Management of acute ischemic stroke. BMJ. 2020;368:l6983.
4. Touze E, Varenne O, Chatellier G, Peyrard S, Rothwell PM, Mas JL. Risk of myocardial infarction and vascular death after transient ischemic attack and ischemic stroke: a systematic review and meta-analysis. Stroke. 2005;36(12):2748-55.
5. Buckley BJR, Harrison SL, Hill A, Underhill P, Lane DA, Lip GYH. Stroke-Heart Syndrome: Incidence and Clinical Outcomes of Cardiac Complications Following Stroke. Stroke. 2022;53(5):1759-63.
6. Merkler AE, Bartz TM, Kamel H, Soliman EZ, Howard V, Psaty BM, et al. Silent Myocardial Infarction and Subsequent Ischemic Stroke in the Cardiovascular Health Study. Neurology. 2021;97(5):e436-e43.
7. Pana TA, Wood AD, Mamas MA, Clark AB, Bettencourt-Silva JH, McLernon DJ, et al. Myocardial infarction after acute ischaemic stroke: Incidence, mortality and risk factors. Acta Neurol Scand. 2019;140(3):219-28.
8. Boulanger M, Bejot Y, Rothwell PM, Touze E. Long-Term Risk of Myocardial Infarction Compared to Recurrent Stroke After Transient Ischemic Attack and Ischemic Stroke: Systematic Review and Meta-Analysis. J Am Heart Assoc. 2018;7(2).
9. Kang K, Park TH, Kim N, Jang MU, Park SS, Park JM, et al. Recurrent Stroke, Myocardial Infarction, and Major Vascular Events during the First Year after Acute Ischemic Stroke: The Multicenter Prospective Observational Study about Recurrence and Its Determinants after Acute Ischemic Stroke I. J Stroke Cerebrovasc Dis. 2016;25(3):656-64.
10. Alqahtani F, Aljohani S, Tarabishy A, Busu T, Adcock A, Alkhouli M. Incidence and Outcomes of Myocardial Infarction in Patients Admitted With Acute Ischemic Stroke. Stroke. 2017;48(11):2931-8.
11. Mooe T, Eriksson P, Stegmayr B. Ischemic stroke after acute myocardial infarction. A population-based study. Stroke. 1997;28(4):762-7.
12. Li L, Pan Y, Wang M, Jing J, Meng X, Jiang Y, et al. Trends and predictors of myocardial infarction or vascular death after ischaemic stroke or TIA in China, 2007-2018: insights from China National Stroke Registries. Stroke Vasc Neurol. 2021;6(2):214-21.
13. Lee KJ, Kim SE, Kim JY, Kang J, Kim BJ, Han MK, Choi KH, Kim JT, Shin DI, Cha JK, Kim DH. Five?Year Risk of Acute Myocardial Infarction After Acute Ischemic Stroke in Korea. Journal of the American Heart Association. 2021 Jan 5;10(1):e018807. vancouver
14. Ambrose JA, Barua RS. The pathophysiology of cigarette smoking and cardiovascular disease: an update. Journal of the American college of cardiology. 2004 May 19;43(10):1731-7.
15. Pan B, Jin X, Jun L, Qiu S, Zheng Q, Pan M. The relationship between smoking and stroke: a meta-analysis. Medicine. 2019 Mar;98(12).
16.Caldwell M, Martinez L, Foster JG, Sherling D, Hennekens CH. Prospects for the primary prevention of myocardial infarction and stroke. Journal of cardiovascular pharmacology and therapeutics. 2019 May;24(3):207-14.
17. Samanta R, Narayan A, Kovoor P, Thiagalingam A. Influence of BMI on short and long-term outcomes in patients with STEMI and LV dysfunction. Heart, Lung and Circulation. 2020 Mar 1;29(3):361-7.