An Analysis of the Outcome of a Prospective Case Series Involving One-Piece Autologous Tuberosity Grafting for Preservation of Alveolar Ridges.
An Analysis of the Outcome of a Prospective Case Series Involving One-Piece Autologous Tuberosity Grafting for Preservation of Alveolar Ridges.
Arshiya Firdous Mohammadi*
*Correspondence to: Arshiya Firdous Mohammadi, Sri Rajiv Gandhi college of Dental Sciences and Hospital, Banglore, India.
Copyright.
© 2025 Arshiya Firdous Mohammadi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 13 Dec 2024
Published: 18 Jan 2025
An Analysis of the Outcome of a Prospective Case Series Involving One-Piece Autologous Tuberosity Grafting for Preservation of Alveolar Ridges.
Introduction
Post-extractional changes in alveolar ridges, including significant reductions in both horizontal and vertical dimensions, can compromise esthetic and functional outcomes. These changes are particularly pronounced during the first 12 months following tooth extraction, with the majority occurring within the first three months. Preservation of the alveolar ridge, often referred to as socket preservation or alveolar ridge preservation (ARP), aims to minimize these dimensional losses. Various grafting materials and techniques have been explored, with no consensus on the ideal approach.
Autologous bone remains the gold standard for ridge preservation due to its osteogenic, osteoinductive, and osteoconductive properties. This study investigates the effectiveness of a novel one-piece autologous tuberosity graft that combines both hard and soft tissue for socket preservation.
Materials & Methods
Study Design and Participants
This prospective study was conducted at Sri Rajiv Gandhi College of Dental Sciences and Hospital. Seven patients (6 females, 1 male) aged 37–58 years, each requiring extraction of a single-rooted tooth, were included. Exclusion criteria included acute infections, medical conditions contraindicating surgery, and severe psychiatric disorders. Ethical approval was obtained (USJ-2018-65), and informed consent was secured from all participants.
Surgical Procedure
Teeth were atraumatically extracted using piezoelectric inserts and elevators. A dual hard and soft tissue graft was harvested from the maxillary tuberosity using a tissue punch and trephine burr, tailored to fit the extraction socket. The graft was stabilized with absorbable sutures. Follow-ups were conducted at 10 and 21 days post-op, with implant placement occurring four months after extraction.
Radiographic and Clinical Evaluations
CBCT scans were obtained pre-extraction and four months post-surgery. The ITK-Snap software was utilized to assess ridge alterations in 3D. Clinical measurements of keratinized gingiva and buccal bone thickness were recorded pre- and post-operatively.
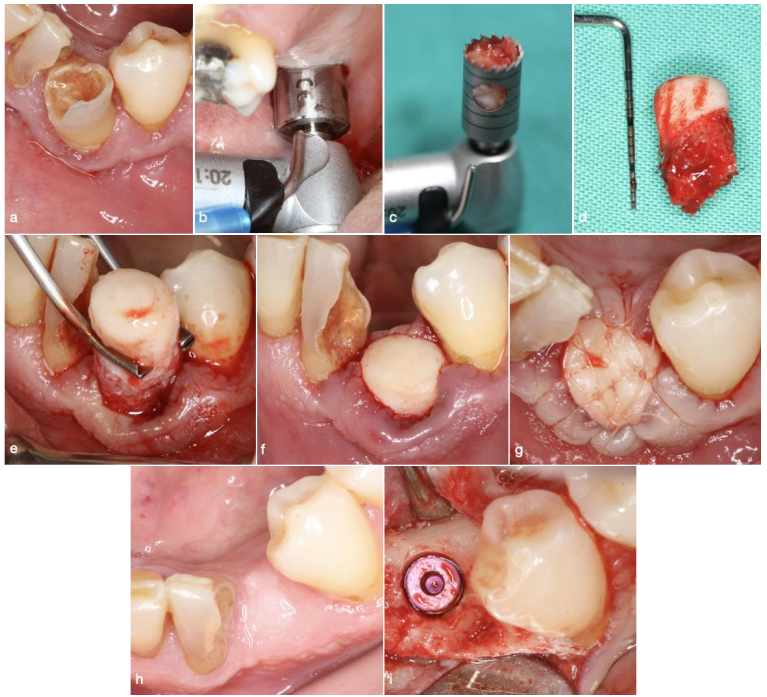
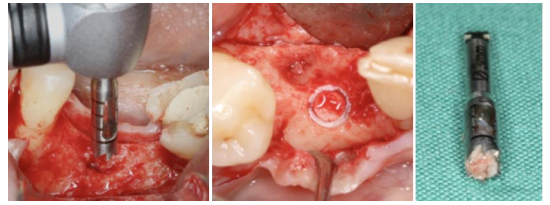
Figure 1 : Pictures of a clinical case using the One Piece autologous tuberosity graft technique (a) tooth #43 to be extracted due to lack of buccal bone and mobility (b) tissue punch being used in the right maxillary tuberosity site (c) bone trephine burr containing the One Piece graft (d) One Piece graft (e) fitting of the graft in the socket (f) placement of the graft inside the socket (g) sutures to stabilize the graft (h) the grafted site 4 months post-op (i) implant placement 4 months post-op.
Clinical Measurements
Clinical measurements were conducted by the same clinician after tooth extraction, including the thickness of soft tissue contouring the tooth on the buccal side and the horizontal width of the socket. The buccal bone plate thickness is divided into existing or missing categories, and the clinical evaluation is correlated with radiography. The presence of the bone plate is divided into thin or thick subcategories. Thin buccal bone plates are less than 0.7mm thick when not visible, while visible ones are thicker than 0.7mm and their width is noted.
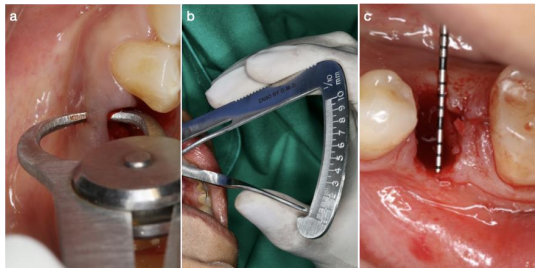
Figure 2 Measurements of (a-b) the thickness of the buccal keratinized gingiva with a dental gauge caliper and (c) the bucco-lingual width of the socket with a periodontal probe.
Four months post-op, implant surgery was performed. After flap elevation, the soft tissue on the buccal side was measured with a dental gauge and the horizontal width of the crest with a periodontal probe (PCP15/11,5, Hu-Friedy®) (Fig. 3).
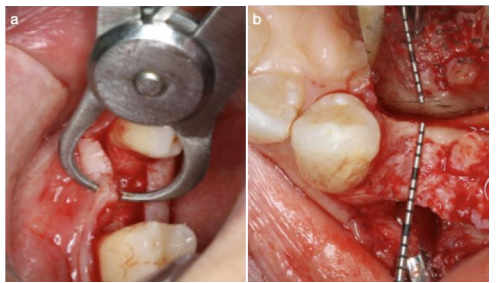
Figure 3 Measurements of (a) the thickness the buccal keratinized mucosa with a dental gauge caliper and (b) the bucco-lingual width of the ridge with a periodontal probe.
Radiographic Measurements
Patients were scanned using the Newtom VGI CBCT machine, with imaging conditions including 110 kv tube voltage, 2.2 to 8.30 mA tube current, 15 x 15 cm field of view, and 0.3mm voxel size. Projection data were collected with a device rotating 360 degrees around patients for 18 seconds. Images were evaluated using the NNT 5.6 software, which re-oriented the images according to three planes: horizontal, vertical, and mesio-distal. T1 and T2 DICOM images were imported and loaded simultaneously into the ITK-snap software, with T1 being the pre-operative CBCT and T2 four months post-operatively. The two CBCT scans were superimposed using the transform and general registration modules, and alignment was manually checked after registration in the three spatial planes. The software allowed a direct comparison of the two scans while maintaining the same alignment.
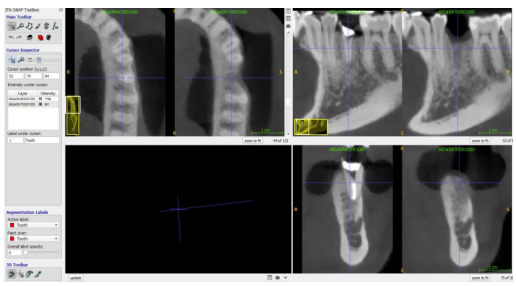
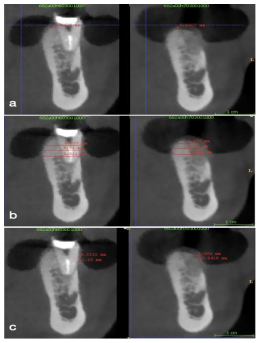
Figure 4 Screenshot of the ITK-Snap software showing the superimposition of the pre-op and post-op CBCT images in the 3 spatial planes.
2D measurements
The study used a cross-sectional 2D slice to measure bone and soft tissue. Bone measurements involved calculating the difference between bone peak levels (T2 – T1) in mm, bucco-lingual width at three different levels (2, 4, and 6 mm) from the most coronal point of the buccal bone, and the difference between T1 and T2 at these levels in mm and %. Soft tissue measurements included the thickness of the mucosa on the buccal side at 2 mm from the most coronal point of the buccal bone, and the difference between T1 and T2 thickness in mm.
Figure 5 Cross sectional images showing the superimposition of T1 and T2. 2D measurements were made (a) Vertical variation of the bone peak between T1 and T2 (b) bucco-lingual width is measured at 3 different levels on both T1 and T2 images (c) thickness of the buccal mucosa at 2 different levels on both T1 and T2 images.
3D volumetric measurements
The study involved volumetric measurements of pre and post-extraction sites, defined by their region of interest (ROI) in three dimensions: apically, mesio-distally, and buco-lingually. Three threshold-based semi-automatic active contour segmentations were performed: tooth segmentation, pre-operative alveolar socket segmentation, and post-operative alveolar bone segmentation. Each segmentation was manually rechecked to remove missing voxel selection. The volume of the T1 and T2 bone was measured using the volumes and statistics tool in the software. All clinical and radiographic measurements were performed by one operator and double checked by an experienced operator in oral and maxillofacial imaging. The duplicate measurements differed by <5%. The STL models were imported into 'Autodesk Netfabb', and a comparative analysis was carried out between the pre and post-operative models, resulting in color-coded figures to identify areas of resorption and bone gain. The results provide valuable insights into the procedure and its potential benefits.
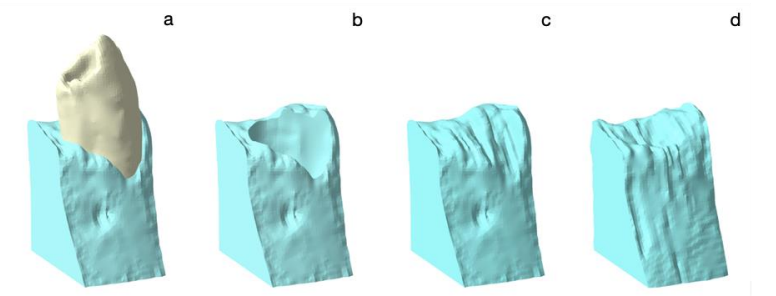
Figure 6 3D segmentations of (a) the tooth and the surrounding alveolar bone (b) the alveolar socket right after extraction (c) the pre-op alveolar socket including the root of the extracted tooth (c) the post-op alveolar bone
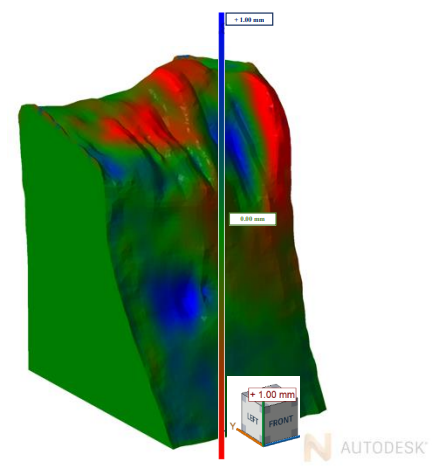
Figure 7 Superimposition of the pre-op and post-op models using the 'Autodesk Netfabb' tool
Histological Evaluation
During the implant placement procedure, bone specimens were harvested from the grafted site using a 3 mm trephine bur (Fig. 8).
Figure 8 Bone specimen harvested from the implant site with a bone trephine burr
The study involved examining bone cores for collagen fiber density (CFD) using a high-precision cutting system and a transmission brightfield/circularly polarized light microscope. The bone cores were rinsed with a cold 5% glucose solution to remove blood and fixed in a 10% buffered formalin solution at pH 7.2 for a week. Dehydration was performed in a series of alcohols before pre-infiltration treatment in a 50% resin/alcohol solution for ten days. The specimens were further processed in four changes of 100% resin and oriented and polymerized under a light source for 8 hours. Sections were prepared along the longitudinal axis of about 50 microns in thickness, ground down to 30±10 microns, and polished with 0.1 micron of alumina particles in a microgrinding system. The sections were stained with a Methylene/toluidine blue solution. The collagen fiber density (CFD) was evaluated using a light microscope equipped with two linear polarizers and a high-resolution CCD-IRIS digital camera. The measurement evaluation was performed using a software package with image capturing capabilities, calibrated for accuracy using 'Calibration Wizard'. The linear remapping of pixel numbers in microns was used to calibrate the distance.
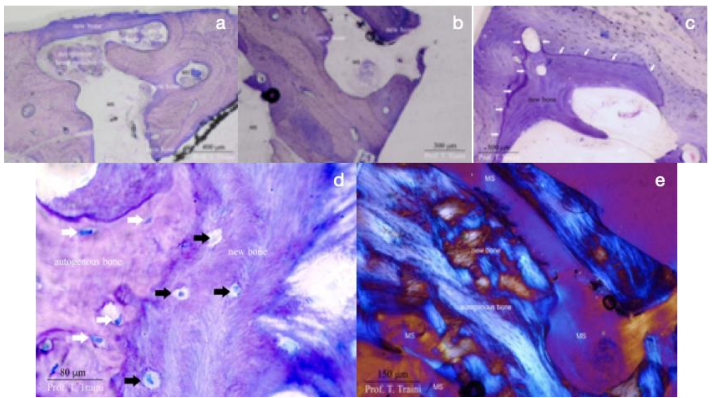
Figure 9 (a-b) Longitudinal section of bone core at 20×; Toluidine-Methylene blue stain. At low-power magnification, some residual particles of the autogenous graft were present, alongside newly formed bone (New bone) as well as marrow spaces (MS). The autogenous bone appears to be covered in some area by a rim of newly formed bone. (c) Small areas of apposition of new bone are visible around the most part of the grafted autogenous bone. White arrows delimit the reversal line of the newly formed bone. (MS) marrow spaces (Toluidine-Methylene blue stain 400×). (d) The evaluation of the interface new bone/grafted autogenous bone at high magnification (x 800) shows the presence of osteocytes (white arrows) in the autogenous grafted bone that survived the transplantation procedure. The new bone area presents several plump vital osteocytes (black arrows). The surviving osteocytes embedded inside the mineralized matrix of the autogenous bone appear to be spindle shaped. (toluidine-methylene blue stain). (e) Under circular polarized light an intimate contact between the new bone and the autogenous grafted bone clearly appears. No difference in the microstructure, mainly the collagen fiber orientation can be seen. (MS) marrow spaces (unstained sample) x100.
Statistical Analysis
The study used the Statistical Package Software for Social Science for statistical analysis, with data expressed as mean ± standard deviation. Kolmogorov-Smirnov tests were used to investigate the normality of the distribution of quantitative variables. The Wilcoxon test was used to compare pre- and post-operative bone volume, and the One-Sample t test was used to compare bone variation with the theoretical value of 0 (no variation). Analysis of variance was conducted to compare bone volume variation and bone resorption rate based on the thickness of the buccal bone plate. Friedman tests were used to compare horizontal linear measurements between levels (2mm, 4mm, and 6mm). Kruskal-Wallis tests and variance analysis followed by Tukey's multiple comparisons were used to compare variations between types of buccal bone plates. The Wilcoxon test was used to compare the width of the bucco-lingual bone and the thickness of the buccal keratinized mucosa.
Results
Healing and Complications
All patients exhibited uneventful healing. One patient did not undergo implant placement due to a change in prosthetic treatment.
Bone Volume Changes
The average reduction in bone volume was 65 ± 76.7 mm³, with a 10.2% volumetric decrease. One site with buccal dehiscence demonstrated a bone volume increase of 66 mm³.
Linear Measurements
- Vertical Changes: Mean vertical loss was 0.026 ± 2 mm, with greater loss observed in sites lacking a buccal bone plate.
- Horizontal Changes: At 2, 4, and 6 mm from the crest, horizontal reductions were 1.5 ± 1.3 mm, 0.47 ± 1.4 mm, and 0.57 ± 0.7 mm, respectively.
Soft Tissue Changes
Keratinized gingiva thickness increased significantly by 1.73 ± 1.12 mm at four months post-op.
Figure 10, 11
Table 1, 2
Please click here to view all figures and tables
Discussion
This study highlights the advantages of using autologous bone grafts, particularly those harvested from the maxillary tuberosity, for socket preservation. The one-piece graft, integrating hard and soft tissue, minimizes ridge resorption and facilitates soft tissue gain. This technique offers several benefits, including reduced cost, minimal donor site morbidity, and shorter healing times compared to xenografts or allografts.
The findings align with previous studies demonstrating that autologous grafts promote superior bone regeneration compared to synthetic materials. Moreover, the inclusion of soft tissue in the graft prevents collapse of the gingiva, maintaining esthetic and functional outcomes.
Conclusion
The one-piece autologous tuberosity graft is a viable solution for alveolar ridge preservation. This technique reduces bone volume loss, promotes soft tissue gain, and ensures optimal conditions for subsequent implant placement. Future studies with larger sample sizes and comparative designs are recommended to validate these findings.
References
1. Schropp L, Wenzel A, Kostopoulos L, Karring T. Bone healing and soft tissue contour changes following single-tooth extraction: a clinical and radiographic 12-month prospective study. Int J Periodontics Restorative Dent. 2003 Aug;23(4):313–23.
2. Tan WL, Wong TLT, Wong MCM, Lang NP. A systematic review of post-extractional alveolar hard and soft tissue dimensional changes in humans. Clin Oral Implants Res. 2012 Feb;23 Suppl 5:1–21.
3. Araujo MG, Lindhe J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J Clin Periodontol. 2005 Feb;32(2):212–8.
4. Lekovic V, Kenney EB, Weinlaender M, Han T, Klokkevold P, Nedic M, et al. A Bone Regenerative Approach to Alveolar Ridge Maintenance Following Tooth Extraction. Report of 10 Cases. J Periodontol. 1997 Jun;68(6):563–70.
5. Lekovic V, Camargo PM, Klokkevold PR, Weinlaender M, Kenney EB, Dimitrijevic B, et al. Preservation of Alveolar Bone in Extraction Sockets Using Bioabsorbable Membranes. J Periodontol. 1998 Sep;69(9):1044–9.
6. Camargo PM, Lekovic V, Weinlaender M, Klokkevold PR, Kenney EB, Dimitrijevic B, et al. Influence of bioactive glass on changes in alveolar process dimensions after exodontia. Oral Surg Oral Med Oral Pathol Oral Radiol Endodontology. 2000 Nov;90(5):581–6.
7. Iasella JM, Greenwell H, Miller RL, Hill M, Drisko C, Bohra AA, et al. Ridge Preservation with Freeze-Dried Bone Allograft and a Collagen Membrane Compared to Extraction Alone for Implant Site Development: A Clinical and Histologic Study in Humans. J Periodontol. 2003 Jul;74(7):990–9.
8. Pelegrine AA, da Costa CES, Correa MEP, Marques JFC. Clinical and histomorphometric evaluation of extraction sockets treated with an autologous bone marrow graft. Clin Oral Implants Res. 2010 May;21(5):535–42.
9. Kerr EN, Mealey BL, Noujeim ME, Lasho DJ, Nummikoski PV, Mellonig JT. The Effect of Ultrasound on Bone Dimensional Changes Following Extraction: A Pilot Study. J Periodontol. 2008 Feb;79(2):283–90.
10. Yilmaz S, Efeo?lu E, Kiliç AR. Alveolar ridge reconstruction and/or preservation using root form bioglass cones. J Clin Periodontol. 1998 Oct;25(10):832–9.
11. Barone A, Ricci M, Tonelli P, Santini S, Covani U. Tissue changes of extraction sockets in humans: a comparison of spontaneous healing vs. ridge preservation with secondary soft tissue healing. Clin Oral Implants Res. 2012 Jul;n/a-n/a.
12. Sakkas A, Wilde F, Heufelder M, Winter K, Schramm A. Autogenous bone grafts in oral implantology—is it still a “gold standard”? A consecutive review of 279 patients with 456 clinical procedures. Int J Implant Dent. 2017 Dec;3(1):23.
13. Reininger D, Cobo-Vazquez C, Rosenberg B, Lopez-Quiles J. Alternative intraoral donor sites to the chin and mandibular body-ramus. J Clin Exp Dent. 2017;0–0.
14. Araújo MG, Lindhe J. Socket grafting with the use of autologous bone: an experimental study in the dog: Socket grafting with the use of autologous bone. Clin Oral Implants Res. 2011 Jan;22(1):9–13.
15. Younes R, Khairallah CM. The “One Piece” Autologous Tuberosity Graft: A Contemporary Concept in Ridge Preservation. López-López J, editor. Case Rep Dent. 2020 Feb 13;2020:3945076.
16. Iorio-Siciliano V, Blasi A, Nicolò M, Iorio-Siciliano A, Riccitiello F, Ramaglia L. Clinical Outcomes of Socket Preservation Using Bovine-Derived Xenograft Collagen and Collagen Membrane Post–Tooth Extraction: A 6-Month Randomized Controlled Clinical Trial. Int J Periodontics Restorative Dent. 2017 Sep;37(5):e290–6.
17. Spinato S, Galindo-Moreno P, Zaffe D, Bernardello F, Soardi CM. Is socket healing conditioned by buccal plate thickness? A clinical and histologic study 4 months after mineralized human bone allografting. Clin Oral Implants Res. 2014 Feb;25(2):e120–6.
18. Jung RE, Philipp A, Annen BM, Signorelli L, Thoma DS, Hämmerle CHF, et al. Radiographic evaluation of different techniques for ridge preservation after tooth extraction: a randomized controlled clinical trial. J Clin Periodontol. 2013 Jan;40(1):90–8.
19. Schneider D, Schmidlin PR, Philipp A, Annen BM, Ronay V, Hämmerle CHF, et al. Labial soft tissue volume evaluation of different techniques for ridge preservation after tooth extraction: a randomized controlled clinical trial. J Clin Periodontol. 2014 Jun;41(6):612–7.
20. Fiorellini JP, Howell TH, Cochran D, Malmquist J, Lilly LC, Spagnoli D, et al. Randomized Study Evaluating Recombinant Human Bone Morphogenetic Protein-2 for Extraction Socket Augmentation. J Periodontol. 2005 Apr;76(4):605–13.