Situs Inversus in a Neonate. About A Clinical Case
Situs Inversus in a Neonate. About A Clinical Case
Vallejo Chaves Saul Hernando 1,2, Gomez Martina Omaira1,2, Portilla Alvarez Fanny1,2, Sanchez Trujillo Sandra1,2
1-Neonatal Intensive Care Unit, UROS Clinic. Neiva, Huila, Colombia.
2-Pediatrics Department, UROS Clinic. Neiva, Huila, Colombia.
*Correspondence to: Dr. Saul Hernando Vallejo Chaves, Pediatrician, Universidad Surcolombiana , Neonatal Intensive Care Unit, UROS Clinic.
Copyright
© 2025: Dr. Saul Hernando Vallejo Chaves. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 27 Jan 2025
Published: 03 Feb 2025
SUMMARY
Situs inversus totalis is a rare condition associated with multiple congenital malformations, the most frequent of which are cardiac; it is also associated with more complex syndromes such as Kartagener's syndrome. In most cases, the condition is a finding after a physical examination for some other reason. It is a rare congenital malformation consisting of the inverted position of the thoracoabdominal organs, which can be total or partial and is frequently associated with syndromes such as Kartagener's syndrome. It requires an early diagnosis and a multidisciplinary approach. It is usually a chance finding, so we should suspect it when respiratory symptoms persist in newborns who are adequately treated and after ruling out other causes that may cause it.
We present the clinical case of a full-term newborn with adequate weight for gestational age with situs inversus totalis detected by echocardiogram and total abdominal ultrasound diagnosed in the first days of extrauterine life; this being the first case reported in our neonatal intensive care unit.
Our goal is to emphasize that early diagnosis completely changes future medical care.
Kartagener syndrome is an autosomal recessive hereditary disease characterized by the association of primary ciliary dyskinesia and the triad situs inversus totalis, chronic sinusitis and bronchiectasis. Its prevalence varies between 1/15,000-1/30,000, but it is estimated that many patients with primary ciliary dyskinesia have not been diagnosed. Its clinical presentation is nonspecific and heterogeneous, and there is no single gold standard test for its diagnosis. This, together with the limitations and unavailability of the tests, causes the diagnosis to be delayed. An adequate diagnosis and early treatment modify the prognosis. In recent years, societies have published diagnostic algorithms for patients with suggestive symptoms. Therefore, it is important to update them and emphasize the need for clinical suspicion in the face of the clinical manifestations of this disease.
KEYWORDS: Kartagener syndrome, primary ciliary dyskinesia, situs inversus, dextrocardia, respiratory distress syndrome in newborns, UROS Clinic, Neiva, Huila, Colombia.
Situs Inversus in a Neonate. About A Clinical Case
Case Presentation
Newborn female referred from San Vicente de Paul Hospital for respiratory distress syndrome and suspected congenital heart disease, this is a 1 day old newborn, the result of the fifth pregnancy, a 41 year old mother, 39 weeks gestation, Grava 5, 2 stillbirths, prenatal check-ups number 5, blood type O positive, mother has gestational diabetes, perinatal screening: HIV negative, VDRL non-reactive, Hepatitis B negative, Toxoplasma IGG positive and IGM negative, delivered by cesarean section due to iterative, born with the following anthropometric parameters: weight 3520 grams, height 50 cm, head circumference 36 cm, chest circumference 35 cm. Spontaneous neonatal adaptation, Apgar 8 - 10 - 10, at birth the baby develops respiratory distress syndrome with a 3-point Silverman - Anderson score, for which reason they are transferred to the newborn unit, non-invasive ventilation is started, a chest x-ray is taken where dextrocardia is evident, for which reason they are referred to the UROS Clinic for comprehensive management in the neonatal intensive care unit. On admission, the patient was hemodynamically stable and showed no signs of low output. He received noninvasive ventilatory support with a high-flow nasal cannula, a FIO2 of 35%, with saturation at target levels. However, during hospitalization, the patient's respiratory condition deteriorated with increased effort, increased retraction, and thoracoabdominal dissociation. Therefore, orotracheal intubation was performed with a 3.5 tube, which was 10 cm from the commissure. Ventilation parameters were adjusted. The patient's progress was favorable. Venous blood gases were taken and showed a pH of 7.32, PO2 35, PCO2 43, HCO3 22, BE -3.9, and lactate of 4.1 with normal serum electrolytes. A chest x-ray was taken and showed a cardiac silhouette on the right and a liver on the left. He ventilated 9 intercostal spaces. without opacities, diagnosis situs inversus totalis , hemodynamically well perfused without low output with blood pressure and heart rate at goals, without indication of inotropic support, heart sounds audible on the right. pulses present. Complementary studies are performed CENTRAL NERVOUS SYSTEM ULTRASOUND study within normal limits, TOTAL ABDOMEN ULTRASOUND An alteration in the position of the abdominal organs is striking, observing the spleen in the right hypochondrium and the liver in the left hypochondrium. Liver of normal shape, size and echogenicity, without focal or diffuse lesions in its parenchyma. Gallbladder and bile duct without alterations. Kidneys, spleen, pancreas and retroperitoneum of normal ultrasound appearance. Empty bladder which prevents assessment of pelvic organs. No masses, collections or free fluid are identified in the abdominal cavity. OPINION: ALTERATION IN THE POSITION OF ABDOMINAL ORGANS (SPLEEN AND LIVER) AN ECHOCARDIOGRAM IS SUGGESTED TO RULE OUT DEXTROCARDIA, ECHOCARDIOGRAM by pediatric cardiology showing CONSERVED SYSTODIASTOLIC FUNCTION OF THE LEFT VENTRICLE TAPSE 9 MM TRICUSPID AND PULMONARY FAILURE PHYSIOLOGICAL OVALE FOSSA 4.1 MM PSPE 34.7 MMHG RESTRICTIVE DUCTUS TOWARDS CLOSURE, DEXTROCARDIA, multidisciplinary evaluations are performed GENETICS patient in stable general condition situs inversus totalis is an alteration that occurs in about 1:10,000 people, with a higher prevalence in men than in women. It is important to rule out whether this occurs in isolation or as part of a more complex syndrome. It is important to keep in mind that 80% of patients have heart disease, which is why a transthoracic echo is required to rule out any anomaly of this type. Additionally, it is important to rule out primary ciliary dyskinesia due to the history of respiratory failure reported by the service. A karyotype with G banding is requested, genomic hybridization is requested (study of deletions and duplications) PEDIATRIC NEUROLOGY patient with high neurological risk due to congenital malformation, with neurological examination with deficit for gestational age, weak suction for gestational age, with echo of the central nervous system without pathological alterations, I request a CEREBRAL MRI Clinical information: situs inversus. Findings: The myelination pattern is normal for the age. The signal from the brain parenchyma does not show alterations. Gray nuclei of the base and thalami without alterations. Subarachnoid space and ventricular system within normal limits for the age. Hypothalamic-pituitary axis, pineal region and corpus callosum of normal appearance. Structures of the posterior fossa without findings of pathological value. Preserved craniovertebral junction. Significant bilateral Oto mastoid occupation. Mucosal thickening in the pneumatized paranasal cavities. Conclusion: Significant bilateral Otomastoid occupation . Intracranial structures within normal limits for age. PEDIATRIC PULMONOLOGY chest x-ray situs inversus, without air leak, adequate lung expansion, OTORHINOLARYNGOLOGY patient with suspected immotile cilia syndrome, currently stable, an electron microscopy of the nasal mucosa is ordered, which can be performed on an outpatient basis, should continue with periodic check-ups by otorhinolaryngology, PEDIATRIC OPHTHALMOLOGY patient with no alterations in the ophthalmological examination, is considered within normal parameters. Control in 6 months , PEDIATRIC CARDIOLOGY newborn with dx of total situs inversus , the echocardiogram showed a systolic pulmonary pressure of 35 mmHg and a restrictive ductus, heart in dextrocardia without dyspnea or cyanosis, finally the patient shows favorable evolution, it is possible to withdraw respiratory support, outpatient follow-up is ordered by different specialties.
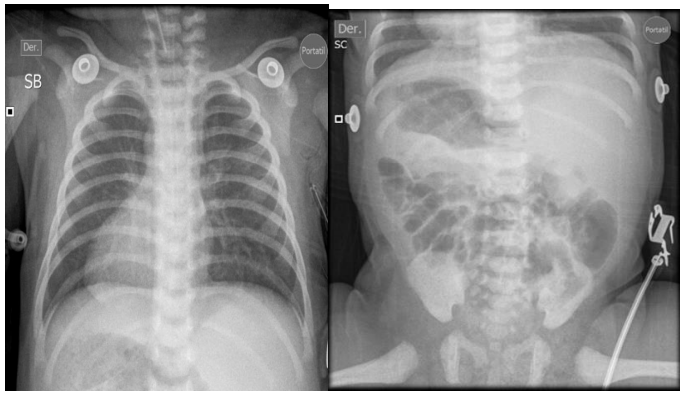
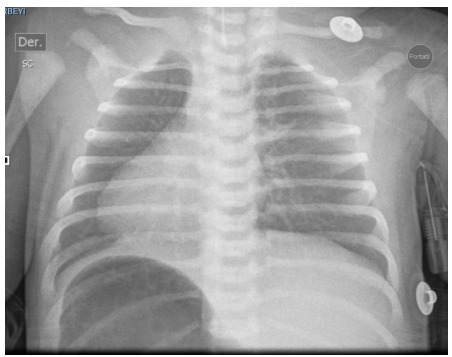
Figure 1. Complete chest-abdomen situs inversus radiograph. Cardiac apex on the right. Liver in the left hypochondrium and gastric fundus in the right hypochondrium.
Fig 3
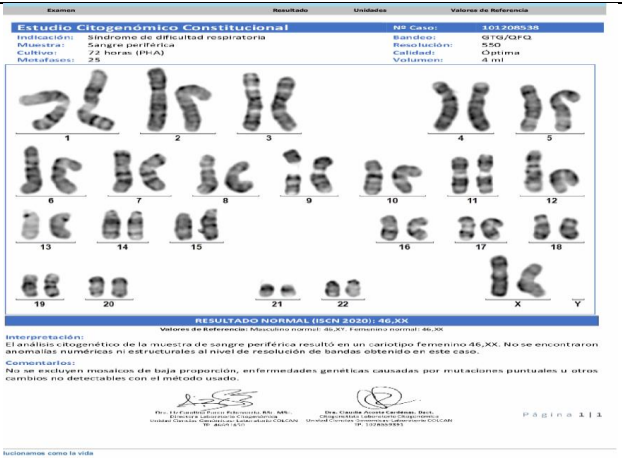
Figure 2 . G banding karyotype / Normal result 46 XX
Discussion
Situs inversus is a rare congenital anomaly (1/10,000) characterized by the abnormal position, with respect to the sagittal plane, of the thoracic and abdominal viscera. It appears in both sexes equally, with no significant differences between races (1)
There are three types of situs: situs solitus , which is the normal position of the body's viscera; situs ambiguous , heterotaxy or isomerism , which is characterized by the abnormal arrangement of the thoracic and abdominal organs across the left-right axis of the body, associated with asplenia or polysplenia ; and situs inversus, which is the inversion of situs solitus , which in turn can be partial, where the heart is in its normal position and the rest of the viscera are inverted, or total, which occurs with dextrocardia and inversion in the position of the intra-abdominal organs. In most cases, inheritance is autosomal recessive, but we can also find, less frequently, some cases with autosomal dominant or X-linked inheritance. (2)
The term dyskinesia refers to the alteration of ciliary movement. It occurs in 1 in every 26,000 to 40,000 live births, approximately half of them will present the classic triad of Kartagener syndrome [3]. Normal ciliary function is critical for respiratory tract defense, sperm motility and normal visceral orientation during embryogenesis [4]. Cilia function may be affected by extrinsic causes (secondary dyskinesia) or may be hereditary with an autosomal recessive transmission pattern in most cases (primary dyskinesia) [4]. The etiology of primary ciliary dyskinesia has been linked to the genetic alteration of the proteins involved in its structure. The DNAI1 and DNAH5 genes are the most related to this disease [5].
Clinical manifestations vary according to age. In the neonatal period, more than 75% of cases present with respiratory distress with an unexplained need for oxygen. In childhood, chronic productive cough, otitis media, rhinorrhea, and recurrent bronchial obstruction are common, wrongly treated as asthma but with poor response to treatment, while in adolescents and adults, bronchiectasis, sinusitis, headache, and infertility in men are more common. [7] In a prospective study published in 2016 by Leigh et al., four specific clinical features in childhood (neonatal respiratory distress with unexplained need for oxygen, wet cough, year-round nasal congestion, and laterality changes) were defined, which, alone or in combination, were predictive of PCD, and had a specificity greater than 96% with at least 3 of these symptoms. [8]
Currently, there is no single gold standard test for the definitive diagnosis of PCD. Classically, the diagnosis has been based on the presence of suggestive symptoms and objective demonstration of structural alterations of the cilium with electron microscopy or ciliary dysfunction by evaluating the frequency and pattern of ciliary beating with high-resolution video. The drawbacks are that they are only performed in specific centers, there may be similar ciliary changes caused by infections or contamination, and up to 30% of patients have cilia with normal ultrastructure. [9] In recent years, genetics has been added to these diagnostic methods, which detect the genes involved in 65% of cases. More than 30 genes have been described; ANAH5 and DNAl1 are the most frequent and attempts are being made to establish a genotype-phenotype correlation. Despite the advances, not necessarily all the mutations found are pathogenic. Therefore, the genetic study is used to confirm the diagnosis in patients with other altered tests or a high index of clinical suspicion. Other diagnostic tests include immunofluorescence and nasal nitric oxide measurement. The accuracy of the latter varies depending on the type of analyzer and the age of the patient (false positive rate of 36% in children under 5 years of age) and is therefore recommended to be used in conjunction with other tests. (9)
Conclusions:
We conclude that situs inversus totalis is a rare entity, whose early diagnosis significantly benefits medical care. Given the large number of associated congenital cardiac malformations, an intentional search for possible conditions through an echocardiogram is mandatory. The rest of the search for associated malformations should be done depending on symptoms and clinical findings, as they have a low incidence. There are no action algorithms for the care of conditions in patients with SIT, from CPR guidelines to surgical protocols. Greater notification of this condition is required in order to develop complete algorithms for the intentional search for associated malformations.
Kartagener's syndrome is a rare disease that has a clinical presentation similar to other respiratory tract conditions. It is important to know its pathophysiology and clinical characteristics in order to establish a timely diagnosis and guarantee specialized multidisciplinary treatment. This clinical entity should be considered when partial or total situs inversus is found in order to determine a diagnosis.
Contributions
The authors actively participated in the diagnosis and treatment of the patient, as well as in the preparation of the case presentation.
Conflict of Interest Statement: None Declared
References
1. Urquia Osorio HO, Discua Flores LJ, Castillo Valenzuela R. Situs inversus totalis and congenital heart disease: a chance diagnosis in an infant with pneumonia. Latin American Federation of Scientific Societies of Medical Students. 2010; 15:85
2. Pandit S, Choudhury S, Das A, Basuthakur S, Das SK. A rare case of Kartagener's syndrome . J Nat Sci Biol Med . 2014 Jan-Jun;5(1):175-7. doi :10.4103/0976-9668.127321
3. Tadesse A, Alemu H, Silamsaw M, Gebrewold Y. Kartagener's syndrome : a case report . J Med Case Rep. 2018 Jan 10;12(1):5. doi :10.1186/s13256-017-1538-2
4. Napolitano C, González C, Iñiguez R, Fonseca X. Primary ciliary dyskinesia: Literature review. Rev. otorhinolaryngol cir cab -neck. 2002; 62: 191-198. Available at: https://www.sochiorl.cl/uploads/15(16).pdf
5. Stern BM, Sharma G. Ciliary Dysfunction (Kartagener Syndrome, Primary Cili- ary Dyskinesia) [Updated 2019 Mar 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm. nih.gov/books/NBK448201/
6. Escribano Montaner A, Armengot Carceller M. Primary ciliary dyskinesia. An Pediatrician Cont . 2013;11(1):38-45.
7. Romero Rubio MT, Rovira Amigo S, Caballero Rabasco MA.Management of the patient affected by primary ciliary dyskinesia. protocol Diagn Ter Pediatrician . 2017;1:423 -37.
8. Leigh MW, Ferkol TW, Davis SD, Lee HS, et al. Clinical Features and Associated Likelihood of Primary Ciliary Dyskinesia in Children and Adolescents. Ann Am Thorac Soc. 2016;13(8):1305-13.
9. Kuehni CE, Lucas JS. Diagnosis of primary ciliary dyskinesia: summary of the ERS Task Force report. Breathe (Sheff). 2017;13(3):166-78.