Effect of Utilizing Piezosurgery in Immediate Implant Placement on Primary Stability, Secondary Stability and Surgery Time: A Case Report
Effect of Utilizing Piezosurgery in Immediate Implant Placement on Primary Stability, Secondary Stability and Surgery Time: A Case Report
Stephanie Khalaf, DDS, MSc *a , Tamara Rbeiz, DDS, MScb, Ghida Lawand, BDS, MSc c , Ibrahim Nasseh, DDS, PhD,d
a Private practice, Beirut , Lebanon
b Clinical Instructor , Department of Periodontology, Faculty of Dental Medicine, Saint Joseph University of Beirut, Beirut , Lebanon.
c ITI Scholar, Department of Oral and Maxillofacial Surgery , College of Dentistry, University of Florida, Gainesville, USA
d Founder and Former Chairman, Department of DentoMaxilloFacial, Radiology, and Imaging, Faculty of Dental Medicine, Lebanese University, Beirut, Lebanon
*Correspondence to: Dr Stephanie Khalaf; Private Practice, Hamra Beirut, Lebanon.
Copyright.
© 2025 Dr Stephanie Khalaf This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 27 Jan 2025
Published: 05 Feb 2025
DOI: https://doi.org/10.5281/zenodo.14880819
ABSTRACT
Immediate Implant Placement (IIP) reduces surgeries and overall treatment time but is a complex procedure with high surgical risks. Achieving primary stability is crucial, depending on factors like bone density and implant bed preparation. This study evaluates piezoelectric surgery for IIP, focusing on stability and surgical time.
A 52-year-old woman underwent IIP with four implants using piezoelectric tips. Implant stability was measured using resonance frequency analysis (RFA) at multiple time points: surgery (T0), 14 days (T1), 21 days (T2), 30 days (T3), 60 days (T4) and one year (T5). Surgical time was recorded and postoperative care included antibiotics and follow-up visits.
No implant failures or severe complications occurred, resulting in a 100% implant survival rate. An early rise in the ISQ values (T1) was noted, demonstarting a change from a decreasing towards an increasing stability pattern as early as 14 days. ISQ values increased over time, indicating improved stability, with substantial stability by 60 days and further consolidation at one year. The mean peak insertion torque was 50 Ncm and average preparation time was 4 minutes.
Piezo surgery, despite requiring more operating time, offers benefits such as precise osteotomies, minimal trauma and enhanced primary and secondary stability, leading to successful IIP outcomes. Further studies are needed to compare its performance with conventional drilling techniques in IIP protocols.
Keywords: Immediate Implant Placement (IIP), Implant Stability, Implant Stability Quotient (ISQ),Piezosurgery, Case Report.
Effect of Utilizing Piezosurgery in Immediate Implant Placement on Primary Stability, Secondary Stability and Surgery Time: A Case Report
Introduction
Immediate Implant Placement (IIP) is a well-documented procedure in the literature. The benefits of performing tooth extraction and implant placement in a single procedure are numerous, including reduced number of surgeries and overall treatment time. This approach also demonstrates implant survival and success rates comparable to other implant placement protocols, whether early or late (1). However, according to the International Team for Implantology’s SAC (straightforward, advanced and complex) classification, the IIP protocol is considered complex, with high surgical and prosthetic risks such as: fracture of the buccal bone during extraction, inability to place the implant in an ideal three dimensional restorative position and the occurrence of marginal mucosal recession.(2)
Achieving primary stability is a fundamental pillar for the success of IIP, which in turns depends on bone density, implant design and implant bed preparation techniques.3 Secondary stability, conversely, is the biological outcome of osseointegration. As primary stability decreases during the early healing period, secondary stability increases gradually due to changes in bone metabolism, shifting from bone resorption to gradual bone formation and maturation. (3)
Implant bed preparation with minimal trauma and prevention of overheating is another pillar for a successful IIP. The conventional implant osteotomy involves using twist drills of increasing diameters, rotating clockwise at speeds between 600 and 2000 rpm, under irrigation.(4) While efficient, traditional drills generate debris, hematoma, heat and can be problematic in IIP bed preparation, where maintaining a proper axis on an inclined surface is crucial.
An alternative technique is the Piezoelectric Implant Site Preparation (PISP), proposed to enhance surgical control, safety and bone healing.(3) Piezosurgery is based on a physical phenomenon where certain ceramics or crystals such as quartz, undergo mechanical vibration and generate cavities. This is capable of dividing solid interfaces such as bone tissue with three main benefits : micrometric cutting with precise operative control,4 selective cutting action on hard tissues and the cavitation effect of the saline solution that improves surgical visibility.(5) Nonetheless, some studies showed that the utilization of PISP necessitates a longer operating time for complete osteotomy compared to conventional drilling techniques.(3) Given the scarcity of studies utilizing piezoelectric surgery in IIP scenarios, this clinical report aims to evaluate its benefit-risk ratio, its effect in achieving primary and secondary stability and its influence on the surgery time.
Material and Methods
A healthy 52-year-old non-smoker woman presented for full mouth rehabilitation. Examination revealed worn maxillary dentition with excessive over-eruption of posterior teeth due to early loss of antagonists, causing an irregular occlusal plane and asymmetrical gingival margins. Cone Beam Computer Tomography showed hopeless teeth 16, 15, 14, 24, and 25 (following the Fédération Dentaire Internationale teeth numbering system) with inversed crown-root ratios and substantial residual bone. The treatment plan included extracting these teeth with IIP on sites 16, 14, 24, and 25. To assess the feasibility of IIP protocol, Kan's classification6 was applied on teeth 14, 24 and 25. They were classified as class II with enough amount of bone apical to the roots to achieve primary stability. As for tooth 16, Milenkovich's classification (7) of the interradicular maxillary septum was used. The septum was "arrow" shape providing a good amount of bone in all dimensions.
Local anesthesia (lidocaine 2% with epinephrine 1:100,000) was administered. Extractions were initiated using piezoelectric tips (Piezomed®, W&H) (EX1, EX2) placed in the sulcus and moved apically and laterally to widen the periodontal ligament space, followed by tooth removal with forceps. For molars, root separation was performed with a carbide bur first. Sockets were thoroughly curetted afterward.
The implant sites were prepared using piezoelectric tips (Piezomed®, W&H) in sequence: I1, I2P, I3P. These tips, diamond-coated for pilot drilling (I1) and smooth for enlarging the preparation (I2P, I3P), oscillate at 22–35 kHz with automatic frequency adjustment. Implants (4.5x10; 4.0x10; 4.0x10; 3.75x12) were placed with the surgical motor (Implantmed®, W&H) and insertion torque (Ncm) was recorded. All implants had the same macrotopography, microtopography, bidirectional cutting threads, conical shape, internal connection, and roxolid material (BLX, Straumann®). The surgical time for each implant was recorded.
Implant stability was measured at the implant level in mesio-distal (MD) and bucco-palatal (BP) directions using resonance frequency analysis (RFA) (SmartPeg 100, type 38, Osstell® Beacon, Osstell®). Measurements were taken at surgery (T0), 14 days (T1), 21 days (T2), 30 days (T3), 60 days (T4), and one year (T5) follow-up when the patient returned for the final prosthesis with provisionals in place. The buccal gap was grafted with xenograft biomaterial (Botiss cerabone®). Implants were immediately loaded using temporary abutments. Occlusion was set to centric relation with no lateral movement. Flaps were sutured around the temporary prosthesis using single and horizontal matrix sutures. Patient was instructed to rinse twice a day (starting the day after surgery) with 0.12% chlorhexidine and received antibiotics (Augmentin 1g) twice a day for 7 days and analgesic medication (Ibuprofen 600 mg) if needed. Implants were evaluated at each visit for mobility, pain, and signs of infection.
Results
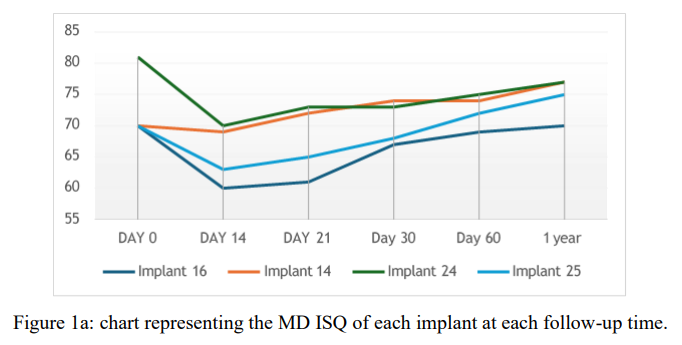
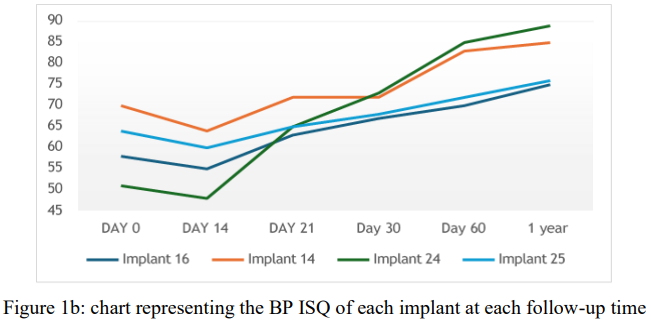
During the follow-up period, no implant failures or prosthetic complications were observed, resulting in a 100% implant survival rate. The tested variables in this study were surgery time and ISQ. Detailed ISQ measurements are presented in Table 1. Significant increases were observed for all implants over time, particularly for implant 24, where BP and MD measurements rose from T0 to T5 (51 to 89; 63 to 85 respectively). For all implants, ISQ decreased during the early healing period. The lowest peak was recorded at T1. From there forward, it continued to increase constantly as presented in Figure 1a,b.
|
Teeth Number |
ISQ |
Day 0 |
Day 14 |
Day 21 |
Day 30 |
Day 60 |
1 year |
|
16 |
BP |
58 |
55 |
63 |
67 |
70 |
75 |
|
16 |
MD |
70 |
60 |
61 |
67 |
69 |
70 |
|
14 |
BP |
70 |
64 |
72 |
72 |
83 |
85 |
|
14 |
MD |
70 |
69 |
72 |
74 |
74 |
77 |
|
24 |
BP |
51 |
48 |
65 |
73 |
85 |
89 |
|
24 |
MD |
81 |
70 |
73 |
73 |
75 |
77 |
|
25 |
BP |
64 |
60 |
65 |
68 |
72 |
76 |
|
25 |
MD |
70 |
63 |
65 |
68 |
72 |
75 |
Table 1: BP and MD ISQ values for all the implants placed, on the day of surgery and at the different follow-up periods
Figure 1a : chart representing the MD ISQ of each implant at each follow-up time.
Figure 1b: chart representing the BP ISQ of each implant at each follow-up time
The preparation time for each implant bed was recorded. The longest time for implant 14 (5.40 min) and shortest for implant 26 (3.00 min). The remaining sites required 4.00 minutes each. The mean preparation time using PISP was 4.00 minutes.
Discussion
This case report aimed to evaluate the impact of PISP on implant primary, secondary stability and assess the operating time within the IIP protocol. As the first case report utilizing piezosurgery in this context, it provides valuable insights into its performance compared to conventional drilling protocols. In fact, PISP can positively affect osseointegration due to favorable biological results, as it decreases pro-inflammatory cytokine activity and promotes osteoprogenitor synthesis and angiogenesis. It also plays a role in protecting local soft tissue structures around the site, while ensuring precision of the osteotomy.(3)
The findings of this report demonstrated an initial decrease in ISQ values from T1 to T2 for all implants which aligns with the transitional phase from primary mechanical stability to secondary biological stability, followed by notable increase in the ISQ , particularly in the BP measurements. This can be attributed to the presence of the buccal gap at time of surgery, leading to a relatively low bone to implant contact (BIC).
The primary stability is influenced by the initial (BIC) and the biomechanical properties of the surrounding bone, whereas the secondary stability is achieved through the biological remodeling and regeneration of surrounding bone, leading to the formation of woven and lamellar bone (8).
Our report observed an early shift toward increasing stability after 14 days (Fig. 1a,b), indicating faster osseointegration and improved implant stability over time. This aligns with studies showing similar results for PISP, whereas the control group saw this shift at 21 days. (3,9,10)
Additionally, a consensus statement noted that PISP greatly outperforms traditional drilling methods in improving secondary stability over three months, but no significant difference was found in achieving primary stability for both techniques.(9)
Another benefit of PISP in IIP is the steady grip of the tip during osteotomy, with no deviation from the initial pilot drill due to micrometric cutting action, enhancing surgical precision. This contrasts with traditional drills, which use rotary movement and are more prone to displacement and deviation.
The preparation time for implant beds using PISP in this IIP protocol was recorded. The variability in preparation time may be attributed to differences in bone quality and quantity, as site 14 presented the largest bone volume requiring osteotomy. While there is no literature measuring this time in IIP scenarios, comparisons can be made with PISP in other implant placement protocols. A randomized clinical trial compared PISP to conventional bone drilling procedures in terms of implant surgery time, finding that PISP took longer (average time 14.6 min ± 1.63) compared to conventional surgical drills (average time 7.5 min ± 1.01).10 Despite this, a recent study stated that even if the difference was statistically significant, it may be clinically inconsequential if surgical or biological benefits outweigh it.(3)
Further studies are needed to confirm these findings and explore the broader applicability of piezosurgery in IIP protocols. It is essential to evaluate the long-term outcomes and compare the performance of piezosurgery with conventional drilling techniques in various clinical scenarios to establish standardized protocols and guidelines.
Conclusion
Piezosurgery is a novel and cutting-edge technique for performing safe and precise osteotomies. The ultrasonic micro-vibrations produced, result in extremely predictable outcomes. Despite the learning curve and increased intraoperative time, piezosurgery proves advantageous in IIP protocols due to improved surgical precision and biological healing. Nevertheless, more studies are needed to better understand the performance of PISP in IIP protocols and to validate its advantages over conventional techniques.
Conflict of Interest Statement
All (co)-authors declare that they have no potential conflicts of interest in relation to the present series.
The present work was self-funded by the authors.
References
1. Gallucci GO, Hamilton A, Zhou W, Buser D, Chen S. Implant placement and loading protocols in partially edentulous patients: A systematic review. Clin Oral Implants Res. 2018 Oct;29 Suppl 16:106–34.
2. Levine RA, Dias DR, Wang P, Araújo MG. Effect of the buccal gap width following immediate implant placement on the buccal bone wall: A retrospective cone-beam computed tomography analysis. Clin Implant Dent Relat Res. 2022 Aug;24(4):403–13.
3. Stacchi C, Troiano G, Montaruli G, Mozzati M, Lamazza L, Antonelli A, et al. Changes in implant stability using different site preparation techniques: Osseodensification drills versus piezoelectric surgery. A multi-center prospective randomized controlled clinical trial. Clin Implant Dent Relat Res. 2023 Feb;25(1):133–40.
4. Scarano A, Carinci F, Lorusso F, Festa F, Bevilacqua L, Santos de Oliveira P, et al. Ultrasonic vs Drill Implant Site Preparation: Post-Operative Pain Measurement Through VAS, Swelling and Crestal Bone Remodeling: A Randomized Clinical Study. Mater Basel Switz. 2018 Dec 11;11(12):2516.
5. Vercellotti T. Technological characteristics and clinical indications of piezoelectric bone surgery. Minerva Stomatol. 2004 May;53(5):207–14.
6. Kan JYK, Roe P, Rungcharassaeng K, Patel RD, Waki T, Lozada JL, et al. Classification of sagittal root position in relation to the anterior maxillary osseous housing for immediate implant placement: a cone beam computed tomography study. Int J Oral Maxillofac Implants. 2011;26(4):873–6.
7. Milenkovic J, Vasiljevic M, Jovicic N, Milovanovic D, Selakovic D, Rosic G. Criteria for the Classification of the Interradicular Septum Shape in Maxillary Molars with Clinical Importance for Prosthetic-Driven Immediate Implant Placement. Diagn Basel Switz. 2022 Jun 10;12(6):1432.
8. Kjaergaard M, Nguyen VG, Brandt J, Pouchet J, Weigl PM. Comparison of Implant Stability Between Conventional Drilling and Piezosurgical Implant Bed Preparation Techniques. J Oral Implantol. 2023 Feb 1;49(1):79–84.
9. Bassi F, Cicciù M, Di Lenarda R, Galindo Moreno P, Galli F, Herford AS, et al. Piezoelectric bone surgery compared with conventional rotary instruments in oral surgery and implantology: Summary and consensus statements of the International Piezoelectric Surgery Academy Consensus Conference 2019. Int J Oral Implantol Berl Ger. 2020;13(3):235–9.
10. Arakji H, Osman E, Aboelsaad N, Shokry M. Evaluation of implant site preparation with piezosurgery versus conventional drills in terms of operation time, implant stability and bone density (randomized controlled clinical trial- split mouth design). BMC Oral Health. 2022 Dec 3;22(1):567.