Recurrent Aphthous Stomatitis
Recurrent Aphthous Stomatitis
Dr. Osama Hmidan*
*Correspondence to: Dr. Osama Hmidan, ENT specialist , Mediclinic Airport Road Hospital , UAE.
Copyright
© 2025 Dr. Osama Hmidan. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 06 February 2025
Published: 15 February 2025
DOI: https://doi.org/10.5281/zenodo.14881930
Abstract
This case highlights the complex relations Recurrent aphthous stomatitis (RAS; aphthae; canker sores) is a common condition characterized by the recurrent appearance of painful ulcers in the oral cavity. These ulcers often affect the mucosal surfaces, and their exact etiology remains incompletely understood. but there is genetic predisposition, with strong associations with interleukin genotypes, and sometimes a family history.In this case report, we describe a 45-year-old male patient with a history of diabetes, hypertension, high levels of workplace stress, and low oral hygiene who presented with recurrent aphthous ulcers in the mouth posterior to the wisdom teeth,with referred otalgia on the same side of the lesion . The clinical management involved addressing the patient’s systemic conditions, improving oral hygiene, and using symptomatic treatments for the ulcers. Management remains unsatisfactory, as topical corticosteroids and most other treatments only reduce the severity of the ulceration, but do not stop recurrence. Must be differentiated from other causes of recurrent ulceration, particularly Behçet disease – a systemic disorder.
Diagnosis is on clinical grounip between systemic health, stress, and oral hygiene in the development and recurrence of aphthous ulcers.
Recurrent Aphthous Stomatitis
Introduction
This case can be useful for clinicians in understanding the potential triggers and comprehensive management of recurrent aphthous stomatitis in patients with underlying systemic conditions like diabetes and hypertension.
Recurrent aphthous stomatitis (RAS), refers to the recurrent formation of small, painful ulcers in the oral mucosa. RAS affects a significant portion of the population and can severely impair quality of life. The exact cause of RAS is multifactorial, with contributions from genetic predisposition, local trauma, immunologic factors, infections, and systemic conditions. While the pathogenesis remains incompletely understood, various factors such as stress, systemic diseases, and poor oral hygiene have been implicated in triggering or exacerbating RAS. This case report describes a patient with diabetes and hypertension who presented with recurrent aphthous ulcers localized posterior to the wisdom teeth, with contributing factors such as stress and low oral hygiene.
Aetiology and pathogenesis
The histopathological changes in the pre-ulcerative stage include infiltration of the epithelium by mononuclear (lymphocytic) cells.Oedema develops, followed by keratinocyte vacuolisation and localised vasculitis causing localised swelling that ulcerates and is infiltrated by neutrophils, lymphocytes, and plasma cells before there is healing and regeneration of the epithelium.
There is a cell-mediated immune response that involves T-cells with generation of
The exact cause of RAS is unknown; however, several factors contribute to its pathogenesis. Common triggers include:
1. Genetic Factors: Family history of RAS is often observed, suggesting a genetic predisposition.
2. Immune Dysfunction: RAS may involve a T-cell mediated immune response, where an abnormal immune reaction leads to mucosal damage.
3. Stress: Psychological stress has been widely reported to exacerbate RAS. It may alter immune function, contributing to the development of aphthous ulcers.
4. Systemic Diseases: Conditions such as diabetes, Crohn’s disease, celiac disease, and HIV/AIDS can predispose patients to recurrent ulceration due to immune system dysfunction or mucosal alterations.
5. Nutritional Deficiencies: Deficiencies in vitamins (especially B12, folate, and iron) have been associated with RAS.
6. Trauma: Mechanical trauma to the mucosa, such as from dental appliances or accidental biting, can trigger ulcer formation.
7. Poor Oral Hygiene: Plaque accumulation and poor oral hygiene contribute to bacterial colonization, which may exacerbate RAS.
For the patient in this case report, contributing factors include systemic conditions like diabetes and hypertension, stress from work, and poor oral hygiene.
Clinical features
The patient, a 45-year-old male, presented with recurrent painful ulcers in the oral cavity, specifically located posterior to the right wisdom teeth. He reported that the Minor RAS (MiRAS) would appear periodically, typically lasting 7-10 days, with a burning sensation that worsened during eating. The patient’s medical history was notable for poorly controlled type 2 diabetes and hypertension, for which he was on pharmacological treatment. His work-related stress was significant, and he admitted to having poor oral hygiene.
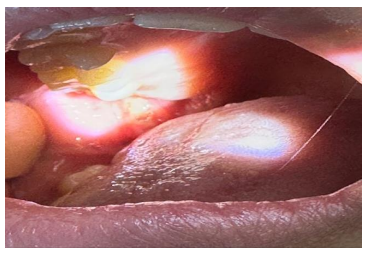
Upon clinical examination, the patient had multiple shallow, round to oval ulcers with a yellowish-white center and erythematous borders. The ulcers were located on the posterior buccal mucosa near the upper wisdom teeth. No systemic signs of infection were noted, and the rest of the oral mucosa appeared normal, without any signs of systemic diseases like systemic lupus erythematosus or HIV.Ear examination normal .
RAS has three main presentations – minor (MiRAS), major (MaRAS) or herpetiform (HU) ulcers.Minor RAS (MiRAS) is the most common, and affects about 80% of patients with RAS
Fig. 1: Minor RAS (MiRAS)
Diagnosis of RAS
Diagnosis of RAS is mainly clinical, based on the patient’s history and presentation. Key diagnostic features include:
- Location: Ulcers located on the non-keratinized mucosal surfaces, often in areas such as the buccal mucosa, soft palate, and tongue.
- Appearance: Shallow, round to oval ulcers with a white or yellowish center and an erythematous border.
- Recurrence: Multiple episodes of ulceration over a period of time.
- Exclusion of other conditions: The absence of systemic signs such as fever, weight loss, or lymphadenopathy suggests that the ulcers are localized rather than part of a systemic illness.
For this patient, the recurrent nature of the ulcers and their location were consistent with RAS. Given his underlying conditions (diabetes and hypertension), and the lack of any other systemic signs, RAS was diagnosed after exclusion of other potential causes, including viral infections and systemic diseases.
There is no specific diagnostic test, but there is a need to exclude other possible causes of recurrent oral ulceration, such as Behçet disease (Fig.2), and possible infection by HIV (Fig.3).
(Fig.2) Behçet disease
Fig.3: HIV
Management of RAS
The assessmeant of the full (complete) blood cell count, red cell folate, and serum levels of ferritin and vitamin B12, which may ,No potential gastrointestinal disease, Negative screening for gluten sensitive enteropathy .
Management of RAS involves both symptomatic relief and addressing the underlying factors that may contribute to its recurrence. The following strategies were used in this case:
1. Symptomatic Treatment: There is no curative treatment for RAS.
- Topical Corticosteroids: The patient was prescribed topical corticosteroids (e.g., triamcinolone acetonide) to reduce inflammation and promote healing of the ulcers.
- Topical Analgesics: Oral gels containing benzocaine or lidocaine were recommended to alleviate pain and discomfort.
- Saltwater Rinses: Warm saltwater rinses were advised to promote healing and prevent secondary infection.
2. Control of Systemic Conditions:
- Diabetes Management: Tight glycemic control was emphasized, with the patient being referred back to his endocrinologist for adjustments to his medication regimen.
- Blood Pressure Management: The patient’s hypertension was controlled with appropriate antihypertensive medications.
3. Improvement of Oral Hygiene:
- The patient was instructed on proper oral hygiene techniques, including the use of a soft-bristled toothbrush, regular flossing, and antimicrobial mouthwashes.
- Regular dental check-ups were recommended to monitor oral health and prevent further trauma or bacterial buildup.
4. Stress Management:
- The patient was advised to manage workplace stress through relaxation techniques, such as deep breathing exercises, meditation, and counseling.
5. Nutritional Support:
- The patient was educated on maintaining a balanced diet rich in vitamins, particularly B12 and folate, to support oral health and reduce the risk of nutritional deficiencies.
Conclusion
This case highlights the multifactorial nature of recurrent aphthous stomatitis, without a combination of systemic health conditions. The poor oral hygiene, and stress contributing to the development and recurrence of oral ulcers. By addressing both local and systemic factors, including improving glycemic control, managing blood pressure, enhancing oral hygiene, and promoting stress management, the patient’s symptoms were significantly reduced, and the recurrence of aphthous ulcers was minimized. This case underscores the importance of a comprehensive approach to managing RAS, with attention to both the medical and lifestyle factors that influence the disease process.
References
(1). S.S. Natah et al. Increased density of lymphocytes bearing gamma/delta T-cell receptors in recurrent aphthous ulceration (RAU) Int J Oral Maxillofac Surg (2000)
2. A. Pedersen et al. Gamma delta T-cell fraction of peripheral blood is increased in recurrent aphthous ulceration
Clin Immunol Immunopathol (1994)
3. R.S. Rogers et al. Lymphocyte-epithelial cell interactions in oral mucosal inflammatory diseases
J Invest Dermatol (1976)
4. I.I. Ship Epidemiologic aspects of recurrent aphthous ulcerations
Oral Surg Oral Med Oral Pathol (1972)