Bilateral Conjunctival Extranodal Marginal Zone Lymphoma of Mucosa-Associated Lymphoid Tissue: A Case Report Highlighting Systemic Therapy as an Alternative and Review of Literature.
Bilateral Conjunctival Extranodal Marginal Zone Lymphoma of Mucosa-Associated Lymphoid Tissue: A Case Report Highlighting Systemic Therapy as an Alternative and Review of Literature.
Dr Praneet Singh Bedi1*, Dr Maheboob Hussain Shaik1
1. Deparment of medical oncology, Max Super specality hospital, Delhi, India.
*Correspondence to: Dr Praneet Singh Bedi, Deparment of medical oncology, Max Super specality hospital, Delhi, India.
Copyright.
© 2025 Dr Praneet Singh Bedi This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 25 March 2025
Published: 01 April 2025
DOI:https://doi.org/10.5281/zenodo.15782025
Abstract:
Conjunctival extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue (MALT lymphoma) is a rare, indolent non-Hodgkin lymphoma that presents with distinct clinical and pathological features. This report describes a 31-year-old male who presented with progressive blurred vision and discomfort in the left eye. Examination revealed a conjunctival mass with a "salmon-patch" appearance, and subsequent histopathology confirmed low-grade MALT lymphoma. Despite recommendations for surgery and radiotherapy, the patient opted for systemic therapy with Rituximab and Bendamustine, achieving complete metabolic remission with significant clinical improvement. This case underscores the importance of early recognition of conjunctival lymphomas and demonstrates systemic therapy as a viable alternative when local treatments are declined.
Keywords: Conjunctival lymphoma, Extra nodal marginal zone lymphoma, Mucosa-associated lymphoid tissue (MALT), Conjunctival MALT lymphoma, Systemic therapy, Rituximab, Ocular lymphoma, non-Hodgkin lymphoma, Conjunctival neoplasms.
Bilateral Conjunctival Extranodal Marginal Zone Lymphoma of Mucosa-Associated Lymphoid Tissue: A Case Report Highlighting Systemic Therapy as an Alternative and Review of Literature.
Introduction
Extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue (MALT lymphoma) is a subtype of non-Hodgkin lymphoma that rarely involves the conjunctiva. Representing only 1.5% of conjunctival tumors, these lymphomas present as painless, salmon-colored masses and are often detected incidentally or during evaluation of visual disturbances. Localized therapies, including surgery and radiotherapy, are commonly employed for treatment and achieve excellent outcomes. However, systemic therapy can be considered when local therapies are not feasible or declined. This case highlights the successful use of systemic therapy in managing conjunctival MALT lymphoma and emphasizes the need for individualized treatment approaches.
Case Report
Clinical History:
A 31-year-old male presented with a three-month history of progressive blurred vision and discomfort in his left eye. He denied systemic symptoms such as fever, night sweats, or weight loss. His medical history was unremarkable, and there was no history of autoimmune conditions or infections.
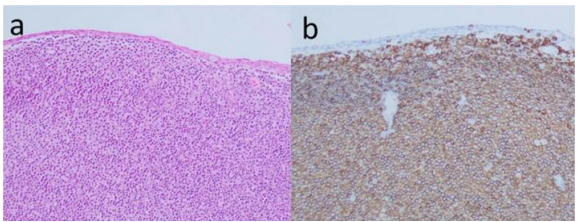
Fig 1 a Haematoxylin and Eosin stain of tissue showing a lymphoid infiltrate within the substantia propria.
b. CD20 IHC shows predominance of positive B cells
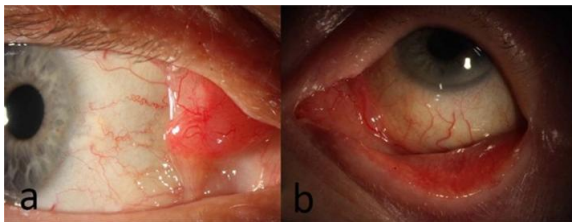
Fig 2: Slit lamp image
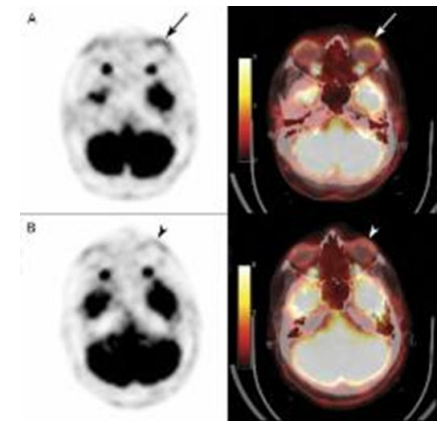
Fig 3: PET CT scan
Ocular Examination :
Visual Acuity: Right eye: 20/20; Left eye: 20/80.
Slit-Lamp Examination: Revealed a gelatinous, "salmon-patch" mass with conjunctival injection in the temporal conjunctiva of the left eye. [Fig.2]
Diagnostic Workup:
Ocular Imaging:
Optical Coherence Tomography (OCT): Demonstrated subconjunctival infiltration with irregular thickening of the left conjunctiva.
Orbital MRI: Identified a well-defined, homogenous mass confined to the conjunctiva with no orbital involvement.
Histopathology:
Conjunctival biopsy revealed dense lymphoid infiltrates composed of small lymphocytes with irregular nuclei. Immunohistochemistry showed positivity for CD20 and Bcl-2, and negativity for CD10, Cyclin D1, and CD3, confirming extranodal marginal zone lymphoma. Ki-67 index was 5-8%. [Fig.1]
Flow Cytometry: Confirmed a monoclonal B-cell population, supporting the diagnosis.
Staging Studies:
PET-CT: Demonstrated FDG-avid soft tissue thickening in the bilateral lower eyelids without systemic spread. [Fig.3]
Treatment Recommendations and Patient Decision:
The patient was advised to undergo localized therapies, including surgical excision and radiotherapy. However, after counseling regarding potential outcomes and side effects, he declined both options.
Systemic Therapy
Systemic therapy was initiated with Bendamustine and Rituximab (BR):
- Initial Therapy: Four 28-day cycles (January to April 2024).
- Response Assessment (April 2024): PET-CT showed a significant reduction in FDG-avid lesions with a Deauville score of 2, indicating complete metabolic remission.
- 2 additional cycles of BR Regimen (May to June 2024).
Follow-Up and Outcomes:
At the six-month follow-up:
Visual Acuity: Improved to 20/25 in the left eye.
Ocular Findings: Complete resolution of the conjunctival mass and injection.
Imaging Studies:
PET-CT (April 2024): Minimal residual soft tissue density in the bilateral lower eyelids with reduced FDG avidity (Deauville score 2).
MRI (May 2024): Resolution of soft tissue swelling and edema in the left conjunctiva.
The patient remained in remission, with no evidence of recurrence or systemic involvement.
PET-CT (Oct 2024): Complete metabolic response
Discussion
Discussion and Literature Review
Conjunctival extranodal marginal zone lymphoma (EMZL) of mucosa-associated lymphoid tissue (MALT) is a rare and indolent form of lymphoma that arises from the conjunctiva. While it represents a subset of ocular adnexal lymphomas (OALs), conjunctival MALT lymphoma accounts for a significant proportion of these cases. Its pathogenesis involves chronic antigenic stimulation, with possible associations with infectious agents such as Chlamydia psittaci and Helicobacter pylori, though this association is less clear in conjunctival cases compared to gastric MALT lymphoma.
Localized vs. Systemic Treatment Approaches
Traditionally, localized conjunctival MALT lymphoma has been managed with radiotherapy, given its efficacy in achieving high local control rates and durable remissions. Radiation doses between 20-30 Gy are commonly employed, with reported complete remission rates exceeding 90%. However, radiotherapy carries risks of ocular complications such as keratoconjunctivitis sicca, cataract formation, and, rarely, radiation retinopathy or optic neuropathy. These potential toxicities make systemic therapy an attractive alternative, particularly for patients with bilateral disease, systemic involvement, or those contraindicated for radiotherapy.
Systemic therapy options include monoclonal antibodies, such as rituximab, and combination chemoimmunotherapy regimens. Rituximab, targeting CD20-positive B cells, has demonstrated efficacy in both localized and systemic EMZL. A study by Conconi et al. reported high overall response rates (ORRs) for rituximab monotherapy in patients with OAL, including conjunctival cases. Rituximab’s favorable safety profile, characterized by low rates of severe adverse effects, makes it particularly suitable for elderly or comorbid patients.
For patients requiring more aggressive therapy, regimens combining rituximab with chemotherapy agents such as bendamustine or CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisone) have shown efficacy. However, these regimens are generally reserved for advanced or refractory disease due to their potential for higher toxicity.
Emerging Therapies and Novel Approaches
Recent advances in understanding the molecular biology of MALT lymphoma have led to the exploration of targeted therapies. Bruton’s tyrosine kinase (BTK) inhibitors, such as ibrutinib, have shown promise in clinical trials for marginal zone lymphoma, though their role in conjunctival MALT lymphoma remains to be fully established. Similarly, therapies targeting the PI3K/AKT/mTOR pathway and immune checkpoint inhibitors are under investigation.
Literature Review of Systemic Therapy in Conjunctival MALT Lymphoma
A review of the literature reveals increasing support for systemic therapy in specific clinical scenarios:
1. Primary Systemic Therapy for Bilateral or Multifocal Disease: Multiple studies have documented the efficacy of rituximab monotherapy or chemoimmunotherapy in patients with bilateral conjunctival MALT lymphoma. For example, studies by Zanni et al. and Stefanovic et al. demonstrated high ORRs and durable remissions with systemic therapy, particularly in cases where radiotherapy was not feasible.
2. Systemic Therapy for Relapsed Disease: Systemic therapy has been a cornerstone in the management of relapsed MALT lymphoma, with rituximab showing consistent activity across multiple studies. Bendamustine-based regimens have also emerged as effective options in the relapsed setting.
3. Combination Approaches: Recent studies have evaluated the combination of radiotherapy with systemic agents, particularly in cases with high tumor burden or partial responses to initial therapy. While these approaches remain investigational, they highlight the evolving paradigm of conjunctival MALT lymphoma management.
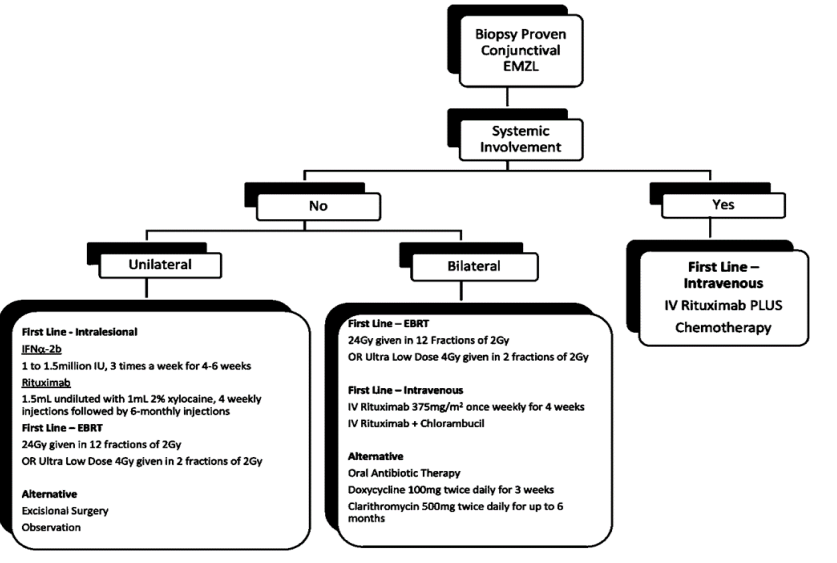
Fig 4
Case Report Context
In the present case, systemic therapy with rituximab + bendamustine was employed as the primary treatment modality, achieving complete remission without significant adverse effects. This case underscores the potential of systemic therapy as a viable alternative to radiotherapy, particularly in patients with risk factors for ocular toxicity or systemic disease involvement.
Conclusion
Conjunctival extranodal marginal zone lymphoma is a rare and treatable malignancy with a generally favorable prognosis when diagnosed early. Local therapies remain the mainstay of treatment, systemic therapy with Rituximab + Bendamustine is a viable alternative in cases where local treatment options are declined. This case highlights the importance of early recognition, patient-centered care, and regular follow-up to ensure optimal outcomes. Increased awareness of conjunctival lymphomas can aid clinicians in providing timely and effective management tailored to individual patient needs.
Conflict of Interest: None
Source of Funding: None
Acknowledgment:
We thank the Department of Medical Oncology at Max Super Specialty Hospital, Delhi, along with the pathology and radiology teams, for their invaluable support in this case. Our gratitude also extends to the patient, their family, and the entire care team whose collaboration made this report possible.
References
Ferreri AJ, Dolcetti R, Dognini GP, et al. Ocular adnexal MALT lymphoma: An updated review. Crit Rev Oncol Hematol.2021;94(3):292-306.
2. Stefanovic A, Lossos IS. Extranodal marginal zone lymphoma of the ocular adnexa. Blood. 2009;114(3):501-510.
3. Conconi A, Franceschetti S, Aprile C, et al. Rituximab in the treatment of patients with extranodal marginal zone B-cell lymphoma of the ocular adnexa. Ann Oncol.2003;14(4):644-650.
4. Tanimoto K, Kaneko A, Suzuki S, et al. Management of localized conjunctival MALT lymphoma: The role of radiotherapy. Am J Ophthalmol. 2005;139(3):486-491.
5. Zinzani PL, Tani M, Trisolini R, et al. Bendamustine and Rituximab in marginal zone lymphomas: A clinical study.Hematol Oncol.2016;34(3):121-128.
6. Kiesewetter B, Raderer M. Antibiotic therapy in extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue. Curr Treat Options Oncol.2013;14(2):249-260.
7. Zucca E, Conconi A, Martinelli G, et al. Final results of the IELSG-19 study: A randomized trial comparing chlorambucil vs. chlorambucil plus rituximab. J Clin Oncol.2003;21(2):103-111.
8. Stefanovic A, Nicholson BT, Lossos IS. Ocular adnexal lymphoma: Epidemiology, clinical presentation, diagnosis, and treatment. Clin Lymphoma Myeloma Leuk. 2009;9(1):89-93.
9. Rasmussen PK, Coupland SE, Zibrandtsen N, et al. Ocular adnexal marginal zone lymphoma: Clinical features and outcomes. Ophthalmology. 2015;122(3):769-776.
10. Kiesewetter B, Willenbacher W. Advanced therapies for marginal zone lymphoma: Beyond first-line therapy. Ann Hematol. 2015;94(1):33-42.
11. Thieblemont C, Cascione L, Conconi A, et al. A clinicopathological study of ocular adnexal marginal zone lymphoma. Lancet Oncol. 2011;12(12):1288-1294.
12. Cheson BD, Fisher RI, Barrington SF, et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma. J Clin Oncol. 2014;32(27):3059-3068.