Occult Primary Neuroendocrine Tumor Presenting as Axillary Lymph Node Metastasis: A Case Report
Occult Primary Neuroendocrine Tumor Presenting as Axillary Lymph Node Metastasis: A Case Report
Dr. Hind Alnassr1, Dr. Elie George Hakme2, Dr. Ahmad Antar3, Dr. Hameed AlAjwad4, Dr. Batool M Al Shehri5, Dr. Naji Fliti 6*
1,2,5,6. Department of General Surgery, Almoosa Specialist Hospital, AlAhsa, Eastern Province, Saudi Arabia.
3. Department of internal Medicine, Division of Oncology , Almoosa Specialist Hospital, AlAhsa, Eastern Province, Saudi Arabia.
4. Department of Pathology, Almoosa Specialist Hospital, AlAhsa, Eastern Province, Saudi Arabia.
*Correspondence to: Dr. Naji Fliti, Department of General Surgery, Almoosa Specialist Hospital, AlAhsa, Eastern Province, Saudi Arabia.
Copyright
© 2025 Dr. Naji Fliti. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 April 2025
Published: 02 May 2025
DOI:https://doi.org/10.5281/zenodo.15386529
Abstract
Neuroendocrine cells (NECs) found throughout the body. These cells exhibit a spectrum of malignant potential, ranging from benign to malignant while the gastrointestinal (GI) tract remains the most frequent primary site for neuroendocrine tumors (NETs), these neoplasms can arise from various other locations, including the pancreas, lungs, and bronchial tree, appendix , colon and rectum .
Clinical case we present exemplifies the diagnostic challenges associated with NETs. It involves a metastasis of a neuroendocrine tumor (NETs) to an axillary lymph node, with unknown primary origin. Our case highlights the potential for NETs to present with occult primary tumors, making diagnosis and treatment planning challenging.
Occult Primary Neuroendocrine Tumor Presenting as Axillary Lymph Node Metastasis: A Case Report
Case Report
A 54-year-old male with no significant past medical history presented to our outpatient clinic with a 10 months history of a right axillary swelling. The swelling has been progressively increasing in size and becoming more painful. He denied any associated skin changes, discharge, fever, night sweats, or loss of appetite.
The patient also reported unintentional weight loss of approximately 7 kilograms over the past 7 months. He denied any history of ?ushing, diarrhea, breathlessness, or generalized lymphadenopathy. Additionally, he reported no prior history of similar swellings or lumps requiring excision and no recent contact with sick individuals.
On physical examination, the patient appeared well-nourished and maintained a good performance status, ECOG 0. Local examination of the right axilla revealed a large, approximately 10 x 10 cm mass with overlying skin erythema and dilated veins.The abdominal examination was unremarkable, with no palpable organomegaly or inguinal lymphadenopathy. A comprehensive lymph node examination of the neck, left axilla,and inguinal regions revealed no palpable masses.
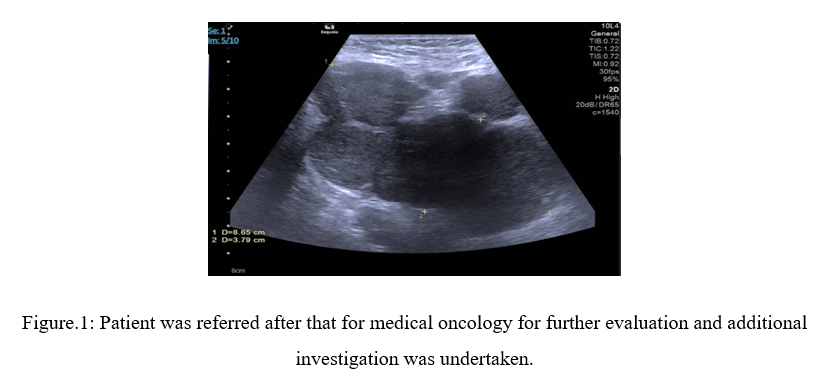
Ultrasound results found Right axillary large hypoechoic solid mass is seen measuring about 8.5x4cm; likely representing amalgamated lymph nodes. It shows increased vascularity inside with high resistivity index measuring 1, suggesting Highly suspicious large amalgamated lymph node mass; for true cut biopsy, see figure 1.
Figure.1: Patient was referred after that for medical oncology for further evaluation and additional investigation was undertaken.
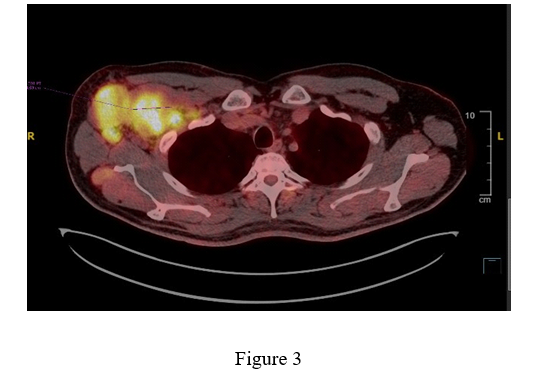
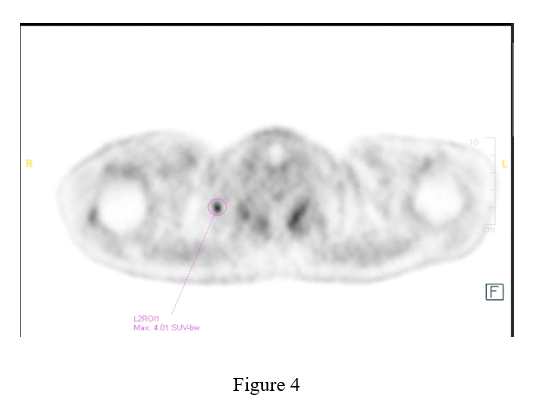
A PET scan of the chest, abdomen, and pelvis was also performed. The scan identified multiple enlarged and abnormally hypermetabolic, matted lymph nodes in the right axillary levels 1 and 2. These nodes showed relatively stable metallic activity, possibly related to prior injections. However, the scan also revealed multiple new lesions extending into the adjacent subcutaneous tissue, potentially involving the thickened skin. Additionally, infiltration of the pectoralis major and minor muscles was observed. The largest right axillary lymph node measured 4.5 x 6.2 cm with a standardized uptake value (SUV) of 9.6.
Importantly, the PET scan did not detect any hypermetabolic lymph nodes below the diaphragm (infradiaphragmatic) or evidence of extranodal hypermetabolic disease .Based on this pattern, the findings are suggestive of stage II lymphoma.
Figure 3, Figure 4
The case was presented at a tumor board, and a decision was made to perform an excisional biopsy of the right axillary lymph node. The final histopathological examination revealed a metastatic poorly di?erentiated neuroendocrine tumor (NEC). Immunohistochemistry testing showed positive staining for Pan-keratin, CamS, Synaptophysin, and Chromogranin. Conversely, the tumor cells were negative for CD20 and CD3 markers.
With following Pathology Microscopic Description
The laboratory received a nodule of soft tissue labelled as right axillary lymph node measuring 2.2 cm in maximum dimension which was sectioned and totally microscopically examined. Histological examination revealed a nodular tumor with large areas of necrosis. The tumor virtually replaced most of the lymph node and is surrounded by thickened fibrotic capsule containing residual lymphoid tissue with presence of subcapsular lymph node sinuses beneath the fibrotic capsule containing tumor cell clusters. The tumor is comprised of sheets and nests of monomorphic cells demonstrating round nuclei with ground glass chromatin pattern, inconspicuous nucleoli, moderate amount of cytoplasm and showing numerous mitotic figures. The subcapsular sinuses and lymphatics outside the lymph node are involved by the tumor cells. A comprehensive panel of immunohistochemistry stains performed with adequate controls revealed tumor cells positive for cytokerain Cam5.2, synaptophysin and chromogranin and are negative for S100, CD45, CD3 and CD20. The morphology and phenotype concluded a diagnosis of metastatic neuroendocrine carcinoma.
Following a comprehensive evaluation, including Pan-endoscopies and thorough dermatologic exam, the definitive diagnosis is metastatic neuroendocrine carcinoma (NEC) involving the right axillary lymph node. Unfortunately, the primary site of origin remains occult. Di?erential diagnoses include a de novo NEC, a less frequent presentation where the cancer originates directly within the right axillary lymph node itself. However, based on the PET scan findings, a soft tissue origin is considered more likely as the PET scan revealed additional lesions extending into the adjacent subcutaneous tissues, and the thickened skin itself could potentially harbor the primary tumor.
The patient was offered treatment with palliative chemotherapy plus Immunotherapy ( Cisplatin etoposide and pembrolizumab) , However he declined any chemotherapy plan and received singly agent Immunotherapy for 3 cycles with no response then he stopped treatment and opted to be on palliative care .
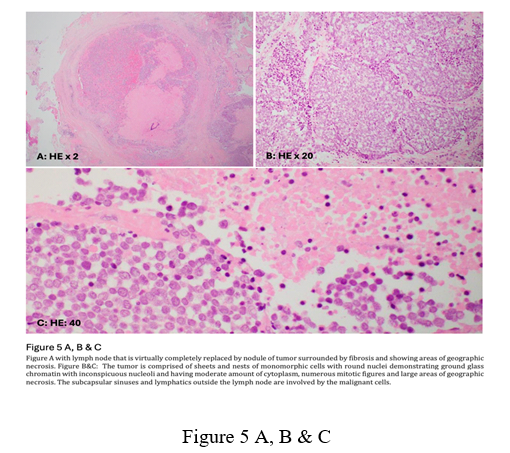
Figure 5 A, B & C
Figure A with lymph node that is virtually completely replaced by nodule of tumor surrounded by fibrosis and showing areas of geographic necrosis. Figure B&C: The tumor is comprised of sheets and nests of monomorphic cells with round nuclei demonstrating ground glass chromatin with inconspicuous nucleoli and having moderate amount of cytoplasm, numerous mitotic figures and large areas of geographic necrosis. The subcapsular sinuses and lymphatics outside the lymph node are involved by the malignant cells.
Discussion
Neuroendocrine tumors (NETs) represent a unique class of malignancies. These tumors arise from neuroendocrine cells scattered throughout the body (1). Notably, they possess the ability to secrete bioactive peptides, which can contribute to symptoms like ?ushing and diarrhea (1). A recent population- based study in Canada revealed a significant rise in NET incidence, increasing from 2.48 to 5.86 per 100,000 people per year between 1994 and 2009 (1).
Neuroendocrine tumors arise in the gastrointestinal tract about 48%, lung 25% and pancreas 9% and they can arise in many other organs, such as the breast, skin, thymus and prostate.
The presentation of neuroendocrine tumors (NETs) with an unknown primary origin is a relatively uncommon event, the incidence of lymph node metastasis from an unidentified primary NET represents less than 5% of all carcinomas arising from unknown primary sites (2).
A review of the literature identified eight cases of neuroendocrine tumors (NETs) within lymph nodes, where the primary tumor origin remained unknown (2). Eusebi et al. reported the possibility of these NETs arising directly from the lymph nodes themselves, based on the presence of epithelial inclusions or anomalous carcinomatous di?erentiation of stem cells within the lymphoreticular system (2).
Our case presentation exhibits a similarity to lymph node metastasis. The patient's condition could be one of two possibilities: either metastasis of a poorly di?erentiated neuroendocrine tumor (NET) from an unknown primary site, or a de novo NET arising directly from the axillary lymphatic tissue or soft tissue itself.
NETs are well di?erentiated and graded as low grade, intermediate grade, and high grade, depending on the mitotic rate and the Ki-67 proliferation index. In contrast, PD-NECs are poorly di?erentiated and high- grade, with a mitotic rate of >20 mitoses/2 mm2 and a Ki-67 proliferation index of >20%.(3)
NET diagnosed based on laboratory ‘ biochemical markers ‘, circulating biomarkers, imaging and histopathology.Computerized tomography, magnetic resonance imaging, somatostatin receptor scintigraphy, and positron emission tomography commonly used for staging workup(2)
The Management of patients with NETs is classified based upon tumor grade and di?erentiation status. Well-di?erentiated (G1) or low-grade (L-grade) NECs often exhibit indolent behavior and are preferentially treated with surgical resection. In contrast, poorly di?erentiated or high-grade (H-grade) NECs demonstrate chemosensitivity to chemotherapy and the first line standard of care is combination of chemotherapy ( etoposide-cisplatin regimen) with or without immunotherapy ( Extrapolated from extensive-stage Small cell lung carcinoma) .( add 3 references as below ) However, the prognosis for patients with poorly di?erentiated NEC remains guarded, with a median overall survival of less than 20% at two years. (2)
The patient was referred to a highly specialized hospital for second opinion. A biopsy was repeated there, with the results being consistent with the initial findings.
Conclusion
Axillary nodal involvement by a soft-tissue neuroendocrine tumor signifies advanced stage disease. Prognosis becomes guarded, though in?uenced by factors such as tumor grade and overall health status. Fortunately, some neuroendocrine tumors demonstrate favorable responses to surgical intervention, targeted therapies, and even chemotherapeutic regimens. Early detection and aggressive management strategies can significantly improve patient outcomes.
The therapeutic cornerstone for patients with both known and occult primary sites of Grade III NETs (NECs) is cisplatin-based combination chemotherapy. Etoposide is frequently incorporated into this regimen due to the established chemosensitivity of these tumors.
Palliative surgical intervention may be warranted to address symptomatic presentations, such as hemorrhage or obstruction, despite its non-curative.
References
1. Raphael, M. J., Chan, D. L., Law, C., & Singh, S. (Eds.). (2017). Principles of diagnosis and management of neuroendocrine tumours. CMAJ, 189(E398-E404). doi: 10.1503/cmaj.160771
2. Dholaria, S. G., Lakhera, K. K., & Patni, S. (2022). Rare case report of neuroendocrine tumor in axilla: Metastasis from unknown primary or de novo? Case Reports in Oncology, 15(1), 388-393. https://doi.org/10.1159/000523989
3. Sano, M., Noguchi, M., Kinoshita, A., Nakamura, M., Koike, K., & Saruta, M. (2022). Poorly differentiated neuroendocrine carcinoma of unknown primary with metastasis to the testis: A case report. Case Reports in Oncology, 15(1), 388-393. https://doi.org/10.1159/000523989
4. Strosberg, J. R., Coppola, D., Klimstra, D. S., Phan, A. T., Kulke, M. H., Wiseman, G. A., ... & Kvols, L. K. (2010). The NANETS consensus guidelines for the diagnosis and management of poorly differentiated (high-grade) extrapulmonary neuroendocrine carcinomas. Pancreas, 39(6), 799-800. doi: 10.1097/MPA.0b013e3181ebb56f
5. Spigel, D. R., Hainsworth, J. D., & Greco, F. A. (2009). Neuroendocrine carcinoma of unknown primary site. Seminars in Oncology, 36(1), 52-59. doi: 10.1053/j.seminoncol.2008.10.003
6. Rudin, C. M., Awad, M. M., Navarro, A., Gottfried, M., Peters, S., Cs?szi, T., ... & Kim, H. R. (2020). Pembrolizumab or placebo plus etoposide and platinum as first-line therapy for extensive-stage small-cell lung cancer: Randomized, double-blind, phase III KEYNOTE-604 study. Journal of Clinical Oncology, 38(21), 2369-2379. doi: 10.1200/JCO.20.0079.