Case Report: Biphenotypic Sinonasal Sarcoma
Case Report: Biphenotypic Sinonasal Sarcoma
Dr.Shuvra Debnath *, Dr. Muhammad Abdullah-Al-Noman 1, Manik Chandra Das 2, Dr. Md. Azizul Hoque Manik 3, Dr. Kamrun Nahar Tania 4
1. Clinical & Radiation Oncologist, National institute of cancer research & hospital, Dhaka.
2. PhD Candidate, Central Queensland University, North Rockhampton, Queensland, Australia.
3. Indoor Medical Officer, Department of Otolaryngology & Head-Neck Surgery, Dhaka Medical College Hospital, Dhaka, Bangladesh.
4. Senior Medical Physicist, National Institute of Cancer Research and Hospital.
*Correspondence to: Dr.Shuvra Debnath, Clinical and Radiation Oncologist, National Institute of Cancer Research and Hospital, Dhaka.
Copyright.
© 2025 Dr.Shuvra Debnath This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 09 June 2025
Published: 16 June 2025
DOI:https://doi.org/10.5281/zenodo.15686561
Abstract
Background: Biphenotypic sinonasal sarcoma (BSNS), a rare malignancy with myogenic and neural differentiation, presents diagnostic and therapeutic challenges due to nonspecific symptoms and histologic complexity.
Case Presentation: A 58-year-old Bangladeshi male presented with 3 months of nasal obstruction, epistaxis, and headache. MRI revealed a 73×55×56 mm nasopharyngeal mass (T4N1M0, AJCC 8th edition). Histopathology showed spindle cells with nuclear atypia, positive for Desmin, MyoD1, Myogenin and S100, confirming BSNS. Post-R1 resection, residual disease prompted adjuvant therapy.
Management: Multimodal therapy included four cycles of ifosfamide/doxorubicin, concurrent chemoradiation (7000 cGy IMRT + weekly chemotherapy), and pazopanib (800 mg/day) for recurrence. Dose reduction (200 mg/day) led to tumor resurgence, necessitating dose escalation (600 mg).
Outcome: Initial regression was followed by recurrence at 1 year, managed surgically and with pazopanib. Toxicity-driven nonadherence highlighted the drug’s dose-dependent efficacy.
Conclusion: This case underscores BSNS’s aggressive nature and the critical role of multimodal therapy (surgery, chemo-radiation, targeted agents) and vigilant follow-up. Pazopanib demonstrates potential in recurrence, but adherence to optimal dosing is vital. Personalized strategies and multidisciplinary collaboration remain pivotal for improving outcomes in this rare malignancy
Case Report: Biphenotypic Sinonasal Sarcoma
Introduction
Sinonasal malignancies are a diagnostic and therapeutic challenge due to the sheer histologic diversity and proximity to vital structures like the orbit, cranial nerves, and brain. Early diagnosis is often confounded by nonspecific symptoms which can be mistaken for benign disease. In addition, there exists a considerable degree of histologic overlap among distinct sinonasal malignancies, making diagnosis on biopsy challenging. One of the most recent sinonasal malignancies described in the latest WHO edition of head and neck tumors is biphenotypic sinonasal sarcoma (BSNS).[1]
Perhaps, most characteristic of BSNS is the presence of both myogenic and neural differentiation. Pathologic descriptions of BSNS include a highly cellular spindle cell neoplasm with monomorphic picture on histology with S-100 and actin positivity on immunophenotyping. It typically shows diffuse or focal positivity for S100 and SMA or MSA. Expression of other muscle markers (MyoD1 and Desmin) are variable. Additional pathological studies including immunophenotyping and fluorescent in situ hybridization (FISH) studies confirm the diagnosis. Clinically, the tumor is slowly progressive with a predilection for upper aerodigestive tract. However, locally aggressive spread may occur in up to half of the affected patients.[2]
The nonspecific nature of the symptoms associated with sinonasal cancer can lead to a delay in diagnosis, which can be detrimental to the patient's prognosis. The most common symptoms are persistent nasal obstruction or congestion, nosebleeds, hearing loss, difficulty swallowing, sore throat, and enlarged lymph nodes in the neck. Patients may present with a combination of these symptoms, which may be confused with other conditions, such as allergies, infections, or other benign causes.[3]
Case Report
A 58-year-old Bangladeshi man presented for consultation with a 3-month history of persistent nasal obstruction or congestion ,occasional nasal bleeding and headache. Upon physical examination, no lymphadenopathies were discovered, and a nasopharyngeal neoplasm was suspected. The initial MRI revealed a 73×55×56 mm mass extending to pterygoid and sphenoid. The MRI also revealed single ipsilateral cervical lymphadenopathy, 25×23 mm .
Initial evaluation work-up included an 18-Fluorodeoxyglucose (18-FDG) PET scan, which showed no sign of distant extension. The patient was classified as T4N1M0 based on the American Joint Committee on Cancer (AJCC) staging, 8th edition. According to ENT consultation, he underwent left lateral rhinotomy with R1 resection.
A biopsy was performed, and the histopathological report revealed spindle-shaped cells with marked nuclear atypia, bizarre nuclei, and frequent mitoses. Immunohistochemical analysis revealed that these spindled- shaped cells expressed desmin, myo D1, myogenin and S 100 but no SMA, CD-34 or STAT 6. which suggested a biphenotypic sinonasal sarcoma. Post operative MRI scan revealed residual of disease but patents improved symptomatically.
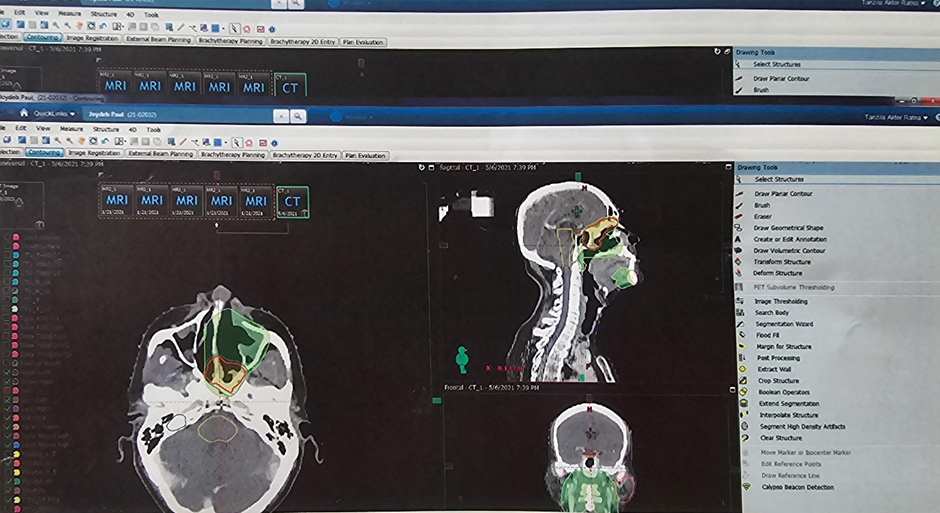
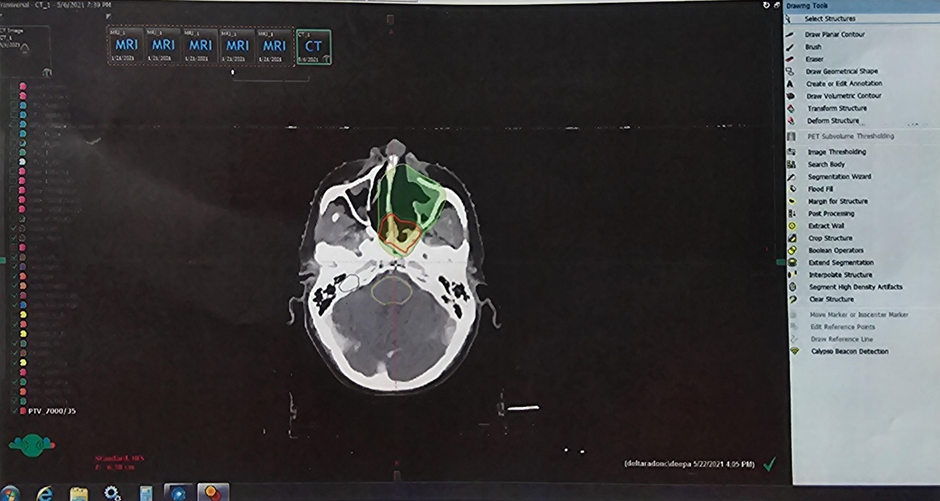
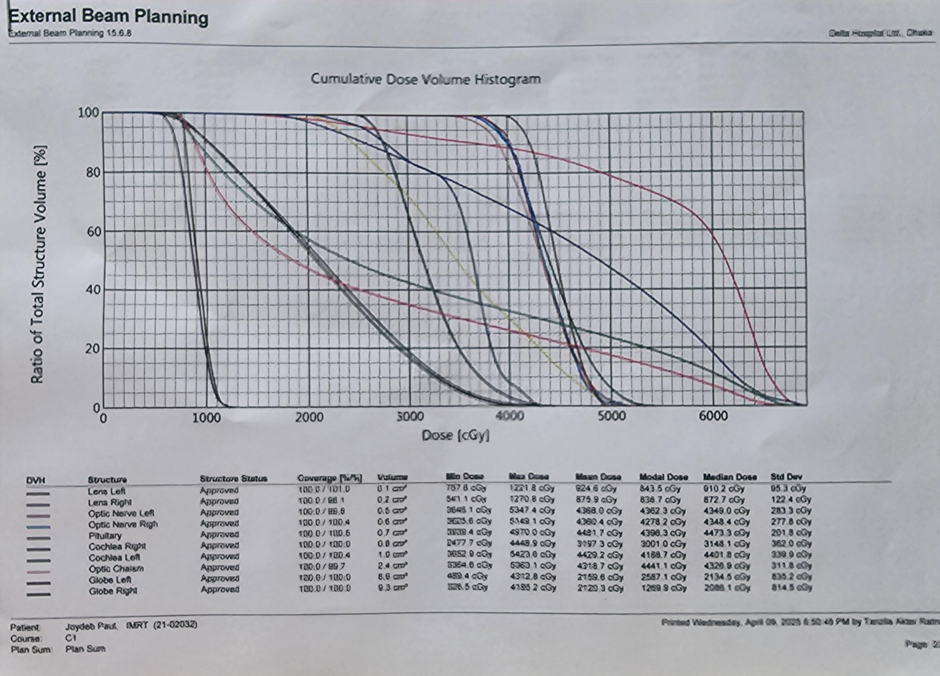
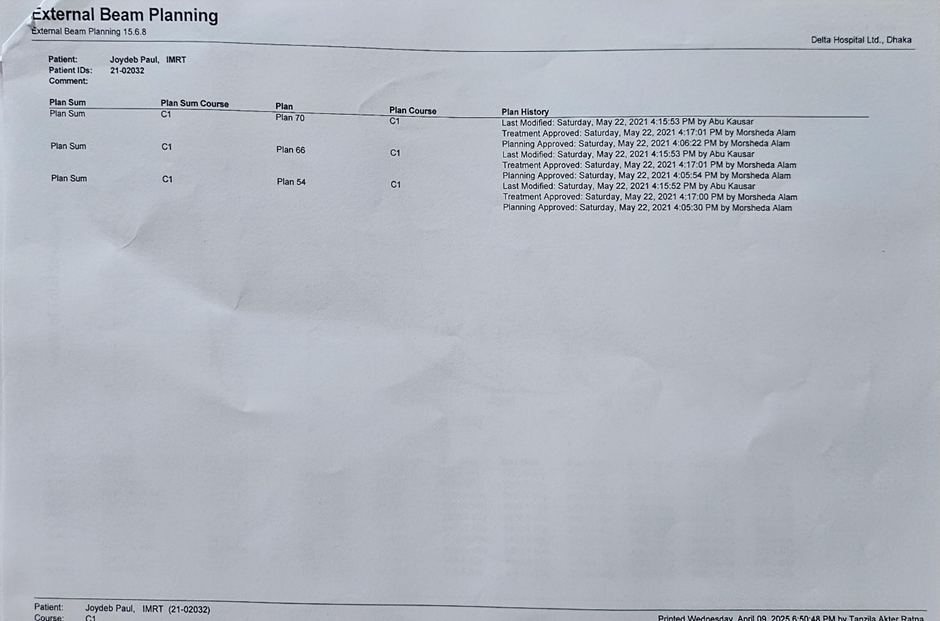
Following the decision of the Head & Neck Tumor Board, the patient was administered four cycles of chemotherapy with ifosfamide and doxorubicin. Following chemotherapy, the patient underwent intensity- modulated radiation therapy (IMRT) with concurrent chemotherapy. He received 7000 cGy IMRT in 35 fraction over 7 weeks along with weekly chemotherapy ( Fig: 1-4). After completing radiotherapy, the patient received an additional four cycles of chemotherapy with the same regimen.
The disease showed a regressive course, and the patient was placed under close follow-up.
During Follow-up, after one year of completion of treatment, both MRI and CT imaging revealed tumor recurrence involving the posterior and left lateral aspect of the nasal fossa, with pansinusitis. Then, the patient was sent back to ENT specialist and underwent a second excision surgery to remove the recurrent tumor. Then he was prescribed oral pazopanib 800 mg daily and showed good response during further follow up visits. Due to toxicity, patient reduced the dose by himself after 16 months. He was taking 200 mg once daily . On subsequent visit after dose reduction, a CT scan was advised which revealed recurrence of tumour again. Now, the dose has been increased to 600 mg with plan of further increase.
Discussion
Biphenotypic sarcomas are aggressive tumors that require multidisciplinary treatment involving surgery, chemotherapy, radiation, and in some cases, targeted therapy. The case highlights the challenges of disease recurrence, emphasizing the need for long-term follow up.
The initial treatment approach –surgery followed by adjuvant chemotherapy, concurrent chemoradiotherapy and a tyrosine kinase inhibitor combinedly led to disease regression. However, recurrence within a year underscores the aggressive nature of biphenotypic sarcomas and the importance of continuous monitoring. The role of radiotherapy in this case is very crucial. Use of pazopanib in recurrent disease has shown a good curative response, as seen in this case.
Further research is needed to define the most effective therapeutic strategy for these rare tumors.
Fig : 1 GTV, CTV and PTV delineation
Fig : 2 : Regions of head and neck getting rsdaiation therapy
Fig :3 : Dose Volume Histogram
Fig 4 : 3 phase radiation planning sum
Conclusion
This case report demonstrates that, multimodal therapy including surgery, chemotherapy, radiotherapy, and targeted therapy, can lead to a favorable outcome in biphenotypic sarcoma of the nasopharynx. Given the high risk of recurrence, long-term follow up and personalized treatment adjustments are crucial for disease control and improved survival rates.
References
1. Victor Sarradin et at., WHO classification of head and neck tumours 2017: Main novelties and update of diagnostic methods. Bull Cancer. 2018 Jun;105(6):596-602. doi: 10.1016/j.bulcan.2018.04.004.
2. Chandala Chitguppi et al., Biphenotypic Sinonasal Sarcoma—Case Report and Review of Clinicopathological Features and Diagnostic Modalities. J Neurol Surg B Skull Base. 2018 Jul 16;80(1):51–58. doi: 10.1055/s-0038-1667146.
3. Jason T Lewiset al., Low-grade sinonasal sarcoma with neural and myogenic features: a linicopathologic analysis of 28 cases. Am J Surg Pathol. 2012 Apr;36(4):517-25. doi: 10.1097/PAS.0b013e3182426886..