Reconstructive Outcomes of Colon Interposition Grafts in Corrosive Esophageal Obstruction: A Tertiary Center Experience.
Reconstructive Outcomes of Colon Interposition Grafts in Corrosive Esophageal Obstruction: A Tertiary Center Experience.
Dr. Muhammad Raza *,
Correspondence to: Dr. Muhammad Raza MBBS, MRCS (Ireland), FCPS (Thoracic Surgery) Thoracic Surgery Specialist, Al-Noor Specialist Hospital, Makkah, Kingdom of Saudi Arabia. ORCID: 0000-0001-6413-8592
Copyright
© 2024 Dr. Muhammad Raza. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 14 June 2025
Published: 21 June 2025
Abstract
Background: Colon interposition is an established treatment for long-segment corrosive esophageal obstruction. This study evaluates our institutional experience with colon interposition using the left colon (based on the left colic artery) in 50 patients, with a focus on early surgical intervention (within 4–6 months of corrosive ingestion).
Methods: A retrospective analysis was conducted on 50 patients (38 females, 12 males; mean age 31.2 years) with corrosive esophageal obstruction who underwent colon interposition using the left colon between January 2018 and December 2024. Patients presented with long-segment, non-dilatable, or multiple esophageal obstructions confirmed by endoscopy and barium swallow. Nutritional status was assessed via serum albumin and body mass index. All patients had a cervical-level anastomosis, with the level measured from the upper incisor (mean 18 cm).
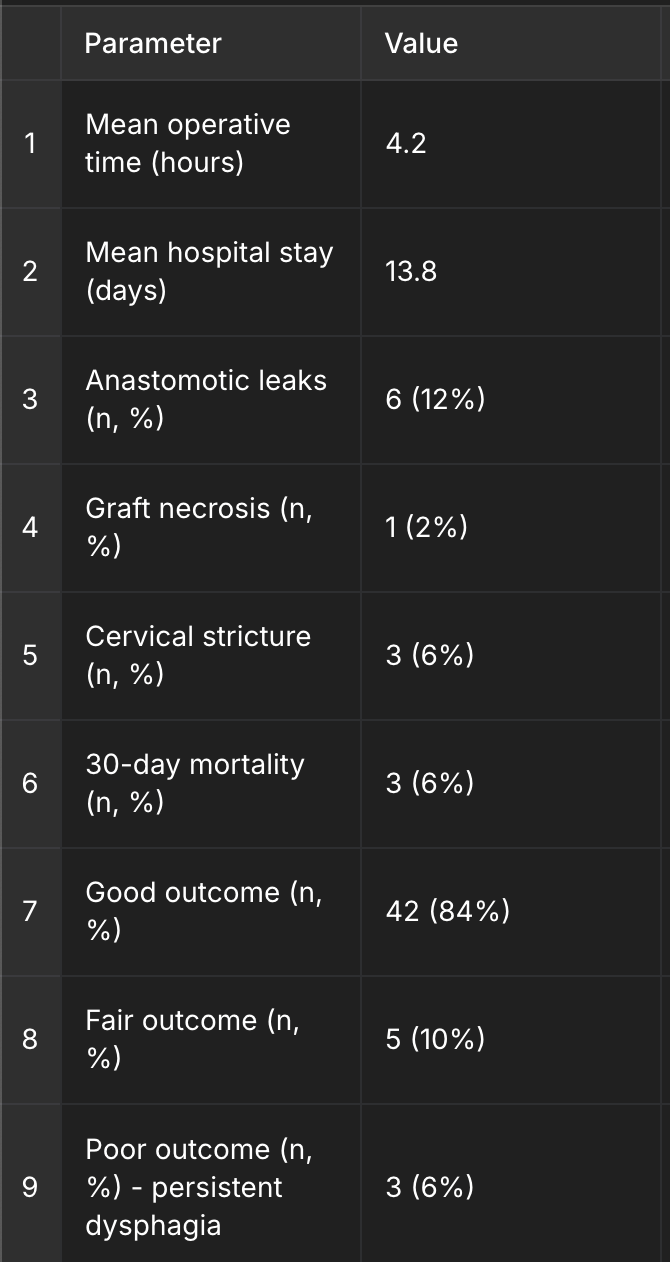
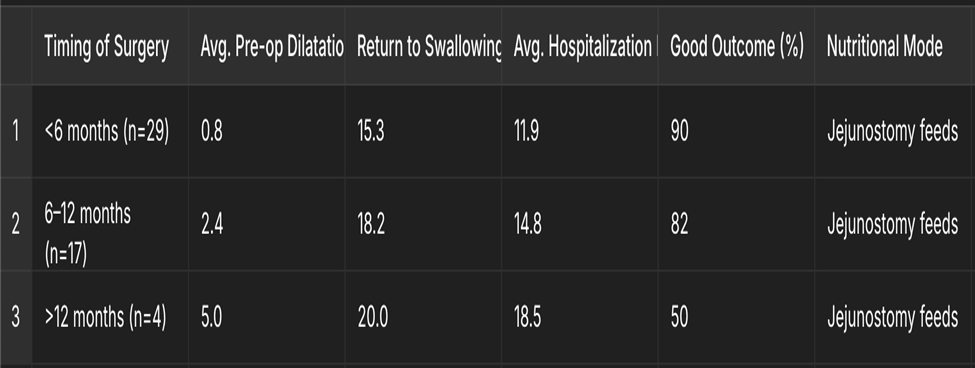
Results: Early surgery (<6 months): 29 patients. Mean operative time: 4.2 hours. Mean hospital stay: 13.8 days. 30-day mortality: 6% (n=3). Anastomotic leak: 12% (n=6). Anastomotic stricture: 3 cases (6%). Graft necrosis: 1 patient. Functional outcomes: 84% "Good," 10% "Fair," 6% "Poor." Early surgery was associated with fewer preoperative dilatations, shorter hospital stay, earlier return to swallowing, and reduced treatment burden.
Conclusion: Colon interposition using the left colon based on the left colic artery is a safe and effective technique for managing corrosive esophageal obstruction. Early surgical intervention improves quality of life, minimizes repeated hospital visits, and standardizes management in suitable candidates.
Keywords: Corrosive ingestion, Esophageal obstruction, Colon interposition, Left colic artery, Early surgery.
Reconstructive Outcomes of Colon Interposition Grafts in Corrosive Esophageal Obstruction: A Tertiary Center Experience.
Introduction
Corrosive ingestion results in devastating injuries to the upper gastrointestinal tract. Esophageal obstruction secondary to caustic injury causes dysphagia, weight loss, and malnutrition. Endoscopic dilatation may be helpful in short, isolated obstructions, but longer or complex obstructions often require surgical reconstruction.
Colon interposition is the preferred reconstructive option when the stomach is unusable or spared for reservoir function. The left colon, based on the left colic artery, provides consistent vascularity, sufficient length, and favorable isoperistaltic orientation. Our study reviews 50 cases of colon interposition, highlighting early versus delayed intervention, with a focus on outcomes and anastomotic levels.
Materials and Methods
Study Design and Setting: This was a retrospective observational study at a tertiary-care teaching hospital, conducted from January 2018 to December 2024. Institutional ethics approval was obtained.
Inclusion Criteria: Patients ≥18 years with corrosive ingestion leading to long-segment or multiple esophageal obstructions, confirmed via barium swallow and endoscopy. All patients underwent colon interposition using the left colon based on the left colic artery. Nutritional status was documented (albumin >3 g/dL preferred).
Exclusion Criteria: Patients with short-segment strictures manageable by endoscopic dilatation, extensive gastric injury, poor nutritional status uncorrected before surgery, and prior upper GI surgeries interfering with conduit mobilization.
Surgical Technique: The left colon was fully mobilized from the descending colon to the transverse and occasionally ascending colon to ensure adequate length. The vascular pedicle was primarily the left colic artery; in two cases, the middle colic artery was used.
Anastomosis:
• Proximal cervical esophagocolic anastomosis (average 18 cm from upper incisor) using single-layer hand-sewn technique (3-0 PDS).
• Distal end-to-side colo-gastric anastomosis on the anterior antrum.
• Side-to-side colocolic anastomosis with GIA stapler.
Route: Substernal in 94% and posterior mediastinal in 6%. Graft orientation: Isoperistaltic in 96%. Anti-reflux strategy: The conduit was tunneled without torsion, and isoperistaltic orientation was maintained. Pylorus was preserved to prevent bile reflux.
Nutrition: All patients received preoperative jejunostomy feeds. Those with poor oral intake were optimized nutritionally over 2–4 weeks.
Assessment of Gastric Status: Endoscopy was used to assess gastric mucosa; patients with extensive gastric involvement were excluded.
Outcome Measures: Primary: Functional swallowing assessed at 6-months via diet tolerance, symptom score, and weight gain. Radiological (barium swallow) follow-up was done in all patients. Secondary: Complications, mortality, preoperative dilatation frequency, and hospital stay.
Results
Demographics: 38 females, 12 males. Mean age 31.2 years. Suicidal ingestion: 84%. Accidental: 16%. Timing of surgery: <6 months (29), 6–12 months (17), >12 months (4).
Complications:
• Anastomotic leak: 6 (12%), managed with drainage and jejunal feeds.
• Graft necrosis: 1 (re-operated).
• Cervical anastomotic stricture: 3 (dilated endoscopically).
• Mortality: 3 (6%), due to sepsis/aspiration.
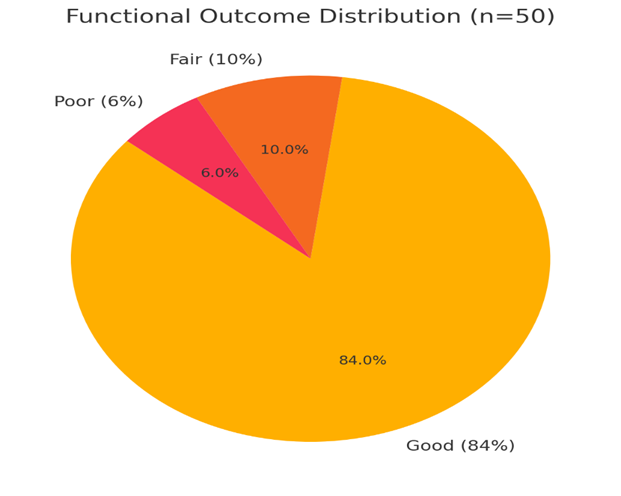
Functional outcomes:
• Good: 42 (84%)
• Fair: 5 (10%)
• Poor: 3 (6%)
Follow-up: Regular for 6–12 months. Barium swallow done at 10–14 days and again at 6 months.
|
Parameter |
Value |
|---|---|
|
Mean operative time |
4.2 hours |
|
Mean hospital stay |
13.8 days |
|
Anastomotic leaks |
6 (12%) |
|
Graft necrosis |
1 |
|
Cervical stricture |
3 |
|
Mortality (30-day) |
3 (6%) |
|
Good outcome |
42 (84%) |
|
Fair outcome |
5 (10%) |
|
Poor outcome |
3 (6%) |
Complications and Outcomes Table — includes detailed breakdowns, clear labeling of the "Poor outcome" category, and accurate complication percentages.
Fig 2, 3
Timing of Surgery Comparison Table — Includes nutritional intake mode (Jejunostomy feeds) and reflects early versus delayed outcomes clearly.
Figure 1
|
Discussion
Our study supports early surgical intervention (<6 months) for corrosive esophageal obstruction as beneficial in terms of reduced hospital admissions, less need for dilatation, and better nutritional recovery. The left colon, due to its consistent anatomy, allows reliable conduit formation with minimal complications.
Cervical anastomosis leaks were effectively managed conservatively in most cases. The functional outcome was superior in patients operated earlier. Gastric preservation allowed physiological continuity and minimized reflux. Nutritional pre-optimization was critical in surgical recovery.
Conclusion
Colon interposition using the left colon is safe and effective. Early surgical timing, nutritional optimization, and standardized conduit formation improve outcomes in patients with corrosive esophageal obstruction.
Future directions include incorporating quality-of-life scores and radionuclide studies for assessing conduit motility.
References
1. Ananthakrishnan, N., Parkash, S., & Kate, V. (2011). Colon as esophageal substitute: Isoperistaltic versus antiperistaltic transpositions. Diseases of the Esophagus, 24(6), 438–443. https://doi.org/10.1111/j.1442-2050.2010.01168.x
2. Knezevic, J. D., Radovanovic, N. S., Stojakov, D., & Krivokapic, Z. V. (2007). Colon interposition for esophageal replacement: A 20-year single institution experience. Diseases of the Esophagus, 20(6), 530–534. https://doi.org/10.1111/j.1442-2050.2007.00746.x
3. Munoz-Bongrand, N., El Bechwaty, M., Valleur, P., & Parc, R. (2005). Colon interposition for esophageal replacement: Current indications and long-term results. Annals of Surgery, 241(2), 324–330. https://doi.org/10.1097/01.sla.0000154264.72712.a8
4. Ogunleye, A. O., Bandele, E. O., & Aremu, T. O. (2012). Corrosive esophageal injury: A review of 36 cases. Nigerian Journal of Surgery, 18(3), 139–142. https://doi.org/10.4103/1117-6806.103104
5. Wilkins, E. W., & Dexter, S. P. L. (1980). Colon interposition for benign esophageal disease: Long-term results. Annals of Thoracic Surgery, 30(3), 243–248. https://doi.org/10.1016/S0003-4975(10)61397-4
6. Gupta, N. M., & Kaman, L. (2005). Personal perspective on corrosive injuries of the upper gastrointestinal tract. Journal of Gastroenterology and Hepatology, 20(3), 701–706. https://doi.org/10.1111/j.1440-1746.2005.03766.x
7. Hanna, W. C., & Ferri, L. E. (2012). Current status of colon interposition in esophageal reconstruction. Current Opinion in Otolaryngology & Head and Neck Surgery, 20(3), 231–236. https://doi.org/10.1097/MOO.0b013e3283544e89.