Eosinophilic Granuloma of Periodontal Tissues & Corresponding Diagnosis and Treatment Plan Options
Eosinophilic Granuloma of Periodontal Tissues & Corresponding Diagnosis and Treatment Plan Options
Omar A.Kharrat *1, Prof.Abdulqader A.Dbbas 2
1. Sr.Consultant . Omar A.Kharrat Oral Maxillofacial Senior Consultant in PSPC-Qatar, Doctor of Dental Surgery, Oral maxillofacial Surgeon, Qatar.
2. Prof.Abdulqader A.Dbbas DDS-OMFS-Consultant in oral maxillofacial Private sector, Turkey, Arab Board of oral maxillofacial surgery Supervisor, Turkey.
*Correspondence to: Omar A.Kharrat Oral Maxillofacial Senior Consultant in PSPC-Qatar, Doctor of Dental Surgery, Oral maxillofacial Surgeon, Qatar.
Copyright.
© 2025 Omar A.Kharrat This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 28 July 2025
Published: 01 Aug 2025
DOI: https://doi.org/10.5281/zenodo.16793979
Abstract
Eosinophilic Granuloma as a manifestation phase of Histiocytosis X is which is the most common of this rare disease characterized by the proliferation of Langerhans cells, which can affect various organs, including bones, skin, and lymph nodes. The clinical manifestations of LCH vary widely, ranging from localized bone lesions (Eosinophilic Granuloma) to disseminated disease with multi-organ involvement.
Eosinophilic Granuloma of Periodontal Tissues & Corresponding Diagnosis and Treatment Plan Options
Introduction
Langerhans Cell Histiocytosis (LCH), formerly known as histiocytosis X, is a rare hematological disorder characterized by the abnormal proliferation of Langerhans cells—specialized antigen-presenting dendritic cells normally found in the skin, lymph nodes, and bone marrow. This condition predominantly affects infants and young children, with an estimated incidence of 2–5 cases per million people annually. Due to its rarity and nonspecific clinical presentation, early diagnosis poses a challenge, often leading to misdiagnosis as other inflammatory or infectious conditions.
Chief Complaint, Clinical & Surgical Findings
The patient (M.S) a 38-year-old male, presented with a chief complaint of bilateral 1st molars mobility associated with severe bone resorption of his mandible. The reason which pushing patient to visit our hospital, the history of recurrent periodontal curettages of mandible with missing of posterior (37,47,48), also patient have history of diabetes insipidus.
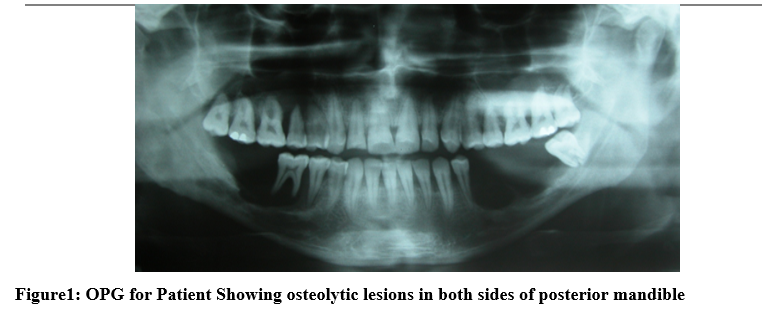
Radiographic examination (figure 1) revealed osteolytic lesions in both sides of posterior mandible, and a biopsy was performed to confirm the diagnosis as Eosinophilic Granuloma.
Figure 1: OPG for Patient Showing osteolytic lesions in both sides of posterior mandible
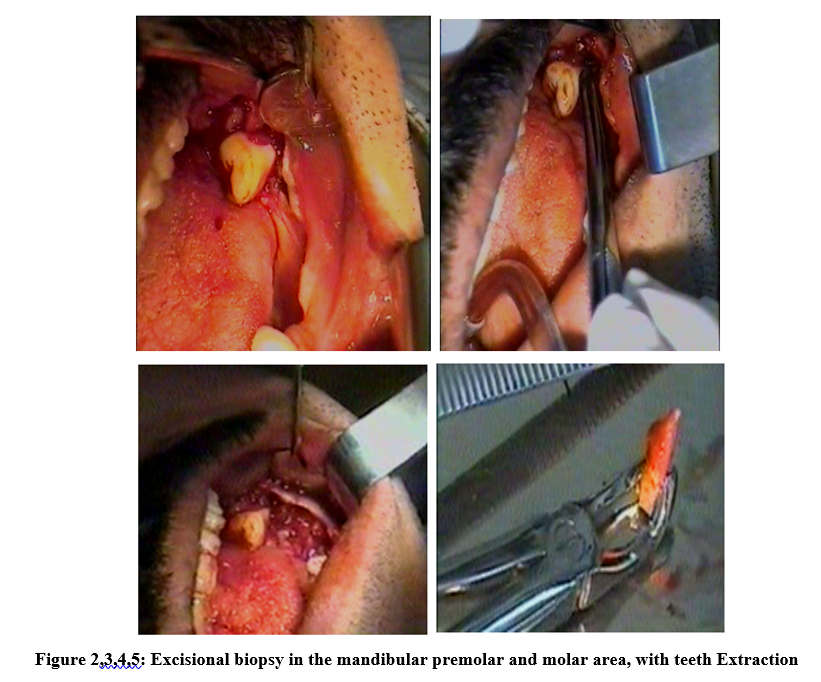
Figure 2,3,4,5: Excisional biopsy in the mandibular premolar and molar area, with teeth Extraction
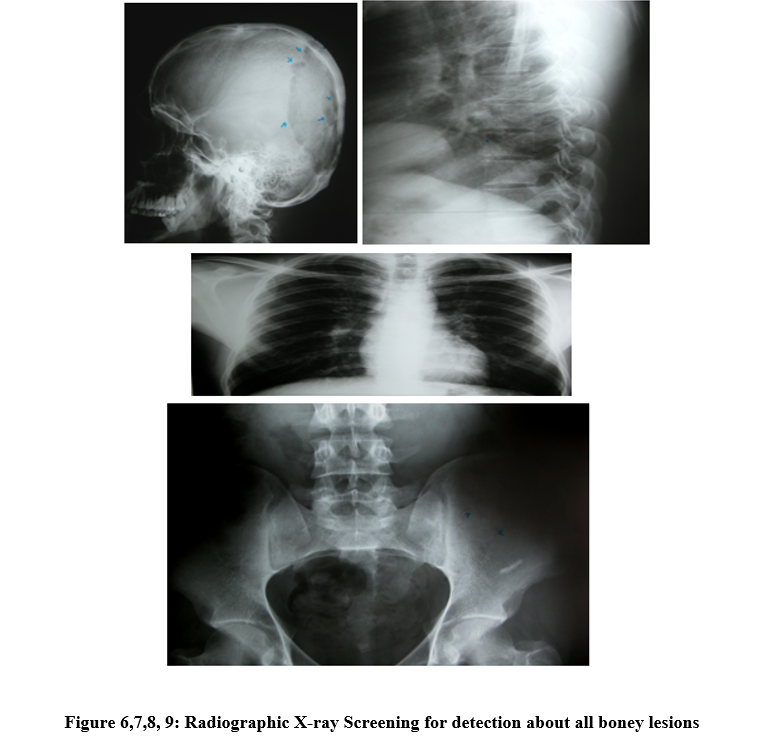
Figure 6,7,8,9: Radiographic X-ray Screening for detection about all boney lesions
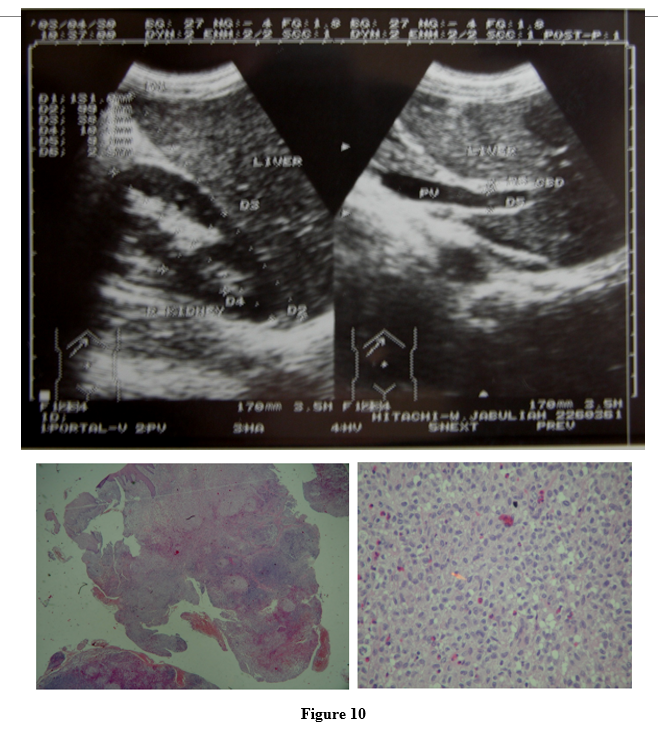
Figure 10
Investigations and deep screening:
The diagnosis of LCH was confirmed through histopathological and immunohistochemical examination, which showed positive CD1a and S100 markers. (Biopsy) (Figure2,3,4,5: excisional biopsy in the mandibular premolar and molar area, with teeth Extraction).
The patient revealed he complained of skin pruritus with rashes on several parts of his body (especially his legs).
Later all further examination done under supervision of Immunity disease specialist, all body screening, x-rays figure 6,7,8,9, abdominal ultrasound (echo) was done figure 10.
Treatment Protocol:
Eventually, the mandibular both sides 1st molar was extracted and an excisional biopsy in the mandibular premolar and molar area was performed (around the 34,35,38 teeth) first, then next visit (around the 44,45,46 teeth). each specimen was placed in a formalin solution and the biopsied lesion (from the end of the tooth's root and in the extracted tooth socket, teeth 35,36,38,45,46 was removed) all was sent to Pathology Department for a histopathologic examination.
See also (Figure2,3,4,5: excisional biopsy in the mandibular premolar and molar area, with teeth Extraction)
Differential Diagnosis:
Macroscopic examination revealed that the specimen consisted of a piece of irregular creamy-brown elastic tissue, microscopic examination showed that the sections contained para-keratinized stratified squamous epithelium with exocytosis and intracellular edema. The connective tissue demonstrated diffused and severe infiltration of chronic inflammatory cells with sheets of histiocytes and numerous scattered eosinophils. Hemorrhaging areas, Russell bodies, bacterial colonies, and a focal area of giant cells were also seen.
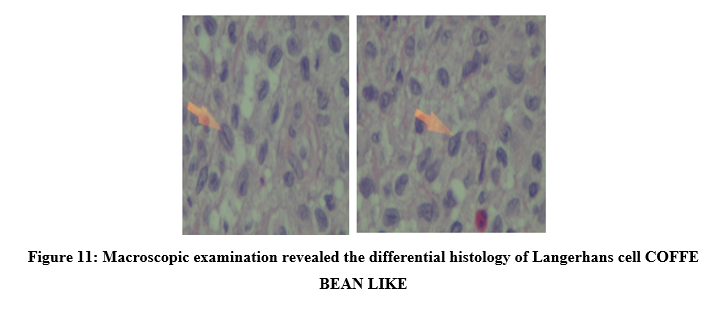
The Langerhans cell contains a moderate amount of homogeneous, pinkish-red granular cytoplasm with clear cell borders. The nucleus is usually folded or striated, giving it a coffee-bean-like appearance. Figure 11
Figure 11: Macroscopic examination revealed the differential histology of Langerhans cell COFFE BEAN LIKE
Further Procedures:
The patient was treated with prednisolone for 45 days, and follow-up examination showed teeth less mobility in comparison to the last check-up,rashes and skin pruritus lowered. The patient will start chemotherapy for the treatment and will be under supervision for complete management.
Etiology and Pathophysiology
Recent advances in molecular genetics have established that LCH is a clonal neoplastic disorder rather than a purely reactive immune process. The key pathogenic feature is the monoclonal proliferation of Langerhans cells driven by somatic mutations in the MAPK signaling pathway:
- BRAF V600E mutation is identified in approximately 60% of cases, indicating a driver mutation that promotes uncontrolled cell growth.
- Other mutations involve genes such as MAP2K1, ARAF, and ERK, further confirming the neoplastic nature of the disease.
These mutations lead to constitutive activation of the MAPK pathway, resulting in increased proliferation, survival, and migration of Langerhans cells, causing tissue infiltration and destruction.
Guidelines about Histiocytosis X
Accurate diagnosis of LCH relies on a combination of clinical, radiological, and histopathological assessments:
Imaging:
• Orthopantomogram (OPG) shows areas of bone loss.
• Computed tomography (CT) scans reveal punched-out, irregular osteolytic lesions with soft tissue involvement.
Histopathology:
• Biopsy reveals proliferation of characteristic Langerhans cells with nuclear grooves and convoluted nuclei.
• The background includes eosinophils, lymphocytes, plasma cells, and multinucleated giant cells.
• Immunohistochemistry confirms the presence of CD1a and Langerin (CD207).
Laboratory Tests:
• Anemia and other nonspecific hematological findings are common.
• Molecular testing for BRAF V600E mutation supports the diagnosis and guides targeted therapy.
Classification of LCH
LCH is classified into three main clinical variants:
1. Letterer–Siwe disease:
Acute, disseminated form primarily affecting infants with multisystem involvement.
2. Eosinophilic granuloma:
Chronic, localized skeletal lesions often seen in children and young adults.
3. Hand–Schüller–Christian disease:
Chronic disseminated form with multiple skeletal and extraskeletal lesions, including diabetes insipidus.
The case discussed falls into the “eosinophilic granuloma” category, characterized by multiple skeletal lesions without systemic involvement.
Outlines of Management:
Treatment strategies depend on the extent of disease:
Localized lesions:
Conservative approaches such as curettage or excision, along with corticosteroids.
Multisystem disease:
Chemotherapy agents like vinblastine, methotrexate, or cytarabine.
Targeted molecular therapies:
BRAF inhibitors (e.g., Vemurafenib) for BRAF-mutant cases.
MEK inhibitors (e.g., Cobimetinib) for non-BRAF mutations.
Prognosis incidence:
• Favorable in localized, single-system disease with early diagnosis.
• More guarded in multisystem or high-risk cases, especially if vital organs are involved.
• Early diagnosis by dental surgeons and multidisciplinary teams improves outcomes.
The Role of Oral Maxillofacial Dental Surgeons
Oral Maxillofacial professionals are pivotal in early detection due to the frequent involvement of the jaw and oral tissues:
• Recognizing nonspecific signs such as gingival swelling, ulceration, and loose teeth.
• Performing biopsies for histopathological diagnosis.
• Collaborating with radiologists and pathologists for comprehensive assessment.
• Contributing to monitoring disease progression and response to therapy.
Conclusion
Langerhans Cell Histiocytosis is a rare but potentially aggressive disease with a complex clinical spectrum. Advances in understanding its molecular basis have led to targeted therapies that have improved patient outcomes. Early diagnosis, especially through the vigilance of dental professionals, and a multidisciplinary approach are crucial for effective management and prognosis.
References:
1. Allen, C. E., Merad, M., & McClain, K. L. (2018). Langerhans cell histiocytosis. Nature Reviews Disease Primers, 4, 13. https://doi.org/10.1038/s41572-018-0004-4
2. Badalian-Very, G., et al. (2010). BRAF mutations are present in Langerhans cell histiocytosis in children and adults. Blood, 116(11), 1919–1923. https://doi.org/10.1182/blood-2010-03-273242
3. Berres, M. L., et al. (2014). BRAF V600E expression in histiocytic disorders. Blood, 124(20), 3174–3184. https://doi.org/10.1182/blood-2014-05-577834
4. Rao, D. G., Trivedi, M. V., Havale, R., & Shrutha, S. P. (2016). A rare and unusual case report of Langerhans cell histiocytosis. PMC, 28479703.
5. Abla O, Egeler RM, Weitzman S. Langerhans cell histiocytosis: Current concepts and treatments. Cancer Treatment Reviews. 2010;36(4):354-359.
6. Ladisch S, Gadner H. Treatment of Langerhans cell histiocytosis—evolution and current approaches. British Journal of Cancer. 1994;70(23):S41-S46.
7. Egeler RM, D'Angio GJ. Langerhans cell histiocytosis. Journal of Pediatrics. 1995;127(1):1-11.
8. Howarth DM, Gilchrist GS, Mullan BP, Wiseman GA, Edmonson JH, Schomberg PJ. Langerhans cell histiocytosis: Diagnosis, natural history, management, and outcome. Cancer. 1999;85(10):2278-2290.