Reversible Splenial Lesion Syndrome, Cytotoxic Lesion of the Corpus Callosum: A Case Report
Reversible Splenial Lesion Syndrome, Cytotoxic Lesion of the Corpus Callosum: A Case Report
Dr Suvarna Dhake MD, DNB, FRCR1*, Dr Rushikesh Naik DNB, FRCR, EDiR2, Dr Mangal Mahajan DNB 3
- Czech Rehabilitation Hospital, Al Ain, United Arab Emirates.
- Burjeel Hospital, Abu Dhabi, United Arab Emirates.
- Burjeel Royal Hospital Al Ain, United Arab Emirates.
*Correspondence to: Dr Suvarna Dhake, Czech Rehabilitation Hospital, Al Ain, United Arab Emirates.
Copyright.
© 2025 Dr Suvarna Dhake, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 27 October 2025
Published: 05 November 2025
Abstract
Reversible splenial lesion syndrome (RESLES) is a rare clinical-radiological syndrome that typically presents with nonspecific central nervous system symptoms. Imaging shows a cytotoxic lesion of the corpus callosum with restricted diffusion and low ADC values and is almost often reversible. Cytotoxic lesions of corpus callosum have been known by variety of terms. The exact pathophysiology is unknown though various mechanisms are proposed. RESLES is seen in multiple clinical settings. Inspite of the diverse etiologies, the MRI findings of cytotoxic edema are same and characteristic for this entity.
Reversible Splenial Lesion Syndrome, Cytotoxic Lesion of the Corpus Callosum: A Case Report
Introduction
Reversible splenial lesion syndrome (RESLES) is a clinical-radiological syndrome of non-specific neurological symptoms with typical MRI findings of well circumscribed round to oval lesion displaying restricted diffusion and low ADC values in the splenium of corpus callosum. Various terms have been proposed for description of this entity including reversible splenial lesions, reversible splenial lesion syndrome (RESLES), Mild encephalopathy with reversible splenial lesion (MERS) and Cytotoxic lesions of the corpus callosum (CLOCCs) [1,2].
The condition may result from several factors, including discontinuation of antiepileptic therapy, infections, high-altitude cerebral edema (HACE), and metabolic abnormalities such as hypoglycemia and hypernatremia [3,4].
RESLES has been associated with various infectious agents notably viruses such as Influenza A, rotavirus, measles, herpesvirus 6, mumps, varicella-zoster virus, adenovirus and bacterial agents such as O157 Escherichia coli-associated hemolytic-uremic syndrome, Legionnaires’ disease [5].
Although RESLES has been reported in all age groups, it is more frequently seen in children [6]. The neurological symptoms that are often reported include dizziness, headache, seizure, disturbance of consciousness, and mental disturbances [7,8]. Usually there is complete recovery without any significant neurological sequelae [9].
We report a child presenting with non-specific neurological symptoms following upper respiratory tract infection with findings of RESLES on imaging as described in literature.
Case Description
A 12-year-old boy had presented to the pediatric outpatient department with rhinorrhea, sore throat and fever. The severity of the symptoms was mild. The fever lasted for two days. The symptoms were treated as an upper respiratory tract infection with an uneventful course. A week following the upper respiratory tract infection, he developed headache with episodes of frequent eye staring and presented to Czech Rehabilitaion Hospital, Al Ain for imaging. The headache was localised to the frontal area with no other visual symptoms or vomiting. No other significant neurological abnormalities were noted on clinical examination.
MRI of the brain with contrast was performed using 1.5 tesla scanner (GE Medical System). An oval well-circumscribed lesion was noted in the splenium of the corpus callosum in the midline (Figure 1). The lesion displayed restricted diffusion with low ADC values (Figures 2 and 3). No evidence of mass effect or perifocal edema was seen. No evidence of abnormal post-contrast enhancement was noted (Figure 4). No lesions are seen in the periventricular white matter and in the subcortical U fibers. In view of the clinical history and morphology of the lesion was read as reversible splenial lesion syndrome (RESLES). The differential diagnosis that were considered included ADEM, multiple sclerosis, encephalitis and glial tumor.
The patient was symptomatically treated as the parents were reluctant for immediate further investigations and short-term follow-up at 3 months was scheduled.
MRI follow-up at 3 months revealed complete resolution of the lesion. No evidence of restricted diffusion or abnormal post-contrast enhancement was observed on the follow-up scan (Figure 5). Evaluation of rest of the brain was unremarkable. The patient was no longer symptomatic for headache or staring episodes.
Discussion
RESLES is an uncommon clinical-radiological syndrome originally reported as Mild encephalopathy with reversible splenial lesion (MERS) in 2004 by Tada et al. Although cases have been reported all over the world, most are reported in Eastern Asian countries [10].
The clinical features of RESLES are non-specific and may include neurological symptoms such as altered mental status, delirious behaviour, seizures, muscle weakness, ophthalmoplegia, and headache [11].
The syndrome is characterised by cytotoxic lesions in the splenium of the corpus callosum, manifesting as areas of low diffusion on diffusion weighted MRI images and low ADC values [12]. These lesions lack post-contrast enhancement and tend to be situated in the midline. Three patterns of involvement of the corpus callosum have been described: (a) round to oval lesion in the centre of splenium (b) Lesion centred in the splenium with extension through the callosal fibres into the adjacent white matter (c) a posteriorly centred lesion with extension into the anterior corpus callosum [13, 14].
Possible mechanisms include intramyelinic oedema due to the separation of myelin layers, interstitial oedema in tightly packed fibres, and a transient inflammatory infiltrate, vascular redistribution, and arginine vasopressin suppression [2,14,15].
Our case highlights typical MRI findings necessary for the diagnosis of this condition in light of non-specific neurological symptoms. The reversibility of neurological as well as imaging findings is most important for distinguishing the syndrome from other neurological conditions that have different management and long-term outcome.
The MRI findings are frequently but not invariably reversible. Follow up MRI studies have revealed complete recovery within 1 month, mostly within 1 week following the neurological recovery [9,16]
Conclusion
Although RESLES is associated with diverse aetiologies, the combination of clinical and imaging findings guide in making specific diagnosis. It is likely that the condition is often not well recognized. Increasing awareness of this entity amongst radiologists can help in avoiding unnecessary investigations and patient anxiety especially since the condition is reversible as opposed to more sinister differential diagnosis.
References
- Starkey J, Kobayashi N, Numaguchi Y, Moritani T: Cytotoxic Lesions of the Corpus Callosum That Show Restricted Diffusion: Mechanisms, Causes, and Manifestations. Radiographics. 2017:562-76. 10.1148/rg.2017160085 - Pubmed
- Takanashi Jun-ichi , Uetani Hiroyuki: Neuroimaging in acute infection-triggered encephalopathy syndromes. Frontiers in Neuroscience. Volume 17 - 2023. 10.3389/fnins.2023.1235364
- Nmadu Y W, Le M M, Aremu O G, et al.: (December 20, 2023). Mild Encephalopathy With Reversible Splenial Lesion (MERS) in a Child With Influenza. Cureus. 15:50838. 10.7759/cureus.50838
- Garcia-Monco JC, Cortina IE, Ferreira E, et al.: Reversible Splenial Lesion Syndrome (RESLES): What's in a Name?. Journal of Neuroimaging, 21. 1:14.
- Bulakbasi N, Kocaoglu M, Tayfun C, Ucoz T: Transient splenial lesion of the corpus callosum in clinically mild influenza-associated encephalitis/encephalopathy. AJNR Am J Neuroradiol. 2006, 27:1983-6.
- Takanashi J, Maeda M, Hayashi M. Neonate showing reversible splenial lesion. Arch Neurol. 2005 Sep;62(9):1481-2; author reply 1482. 10.1001/archneur.62.9.1481.
- Gao, X, Feng, Q, Arif, S, Liaqat, J, Li, B, and Jiang, K. Clinical analysis of reversible splenial lesion syndrome in chinese adults: a retrospective study of 11 cases. Medicine (Baltimore). (2020) 99:e22052. 10.1097/MD.0000000000022052
- Lu, P, Hodes, JF, Zheng, X, and Hu, X. Reversible splenial lesion syndrome with some novel causes and clinical manifestations. Intern Med. (2020) 59:2471–80. 10.2169/internalmedicine.4516-20
- Ka A, Britton P, Troedson C, Webster R, Procopis P, Ging J, et al. Mild encephalopathy with reversible splenial lesion: an important differential of encephalitis. Eur J Paediatr Neurol. 2015;19:377–82.
- Yuan ZF, Shen J, Mao SS, et al.: Clinically mild encephalitis/encephalopathy with a reversible splenial lesion associated with Mycoplasma pneumoniae infection. BMC Infect Dis. 2016, 16:230. 10.1186/s12879-016-1556-5
- Talukder NT, Feezel A, Lankford JE: Mild encephalitis/encephalopathy with a reversible splenial lesion associated with systemic Mycoplasma pneumoniae infection in North America: a case report. J Med Case Rep. 2022, 16:74. 10.1186/s13256-022-03299-6
- Loh, Y., Watson, W.D., Verma, A. and Krapiva, P. (2005: Restricted Diffusion of the Splenium in Acute Wernicke's Encephalopathy. Journal of Neuroimaging. 2005, 15:373-375.
- Jay Starkey, Nobuo Kobayashi, Yuji Numaguchi: and Toshio Moritani RadioGraphics 2017 37: 2, 562-576 Cytotoxic Lesions of the Corpus Callosum That Show Restricted Diffusion: Mechanisms, Causes, and Manifestations.
- Tamanna Yasmin Shena, Umme Kulsum Chy, Amina Sultana, & Mohammad Omar Faruq. (2023). A case of reversible cytotoxic lesion of corpus callosum (CLOCCs) secondary to septic encephalopathy caused by suspected enteric fever. Bangladesh Critical Care Journal, 11(2), 140–141. 10.3329/bccj.v11i2.69149
- Xue J, Zhang Y, Kang J, et al.: A cohort study of mild encephalitis/encephalopathy with a reversible splenial lesion in children. Brain Behav. 11:2306. 10.1002/brb3.2306
- Tada H, Takanashi J, Barkovich A, et al.: Clinically Mild Encephalitis/Encephalopathy with a Reversible Splenial Lesion. Neurology. 2004:1854-8. 10.1212/01.wnl.0000144274.12174.cb - Pubmed
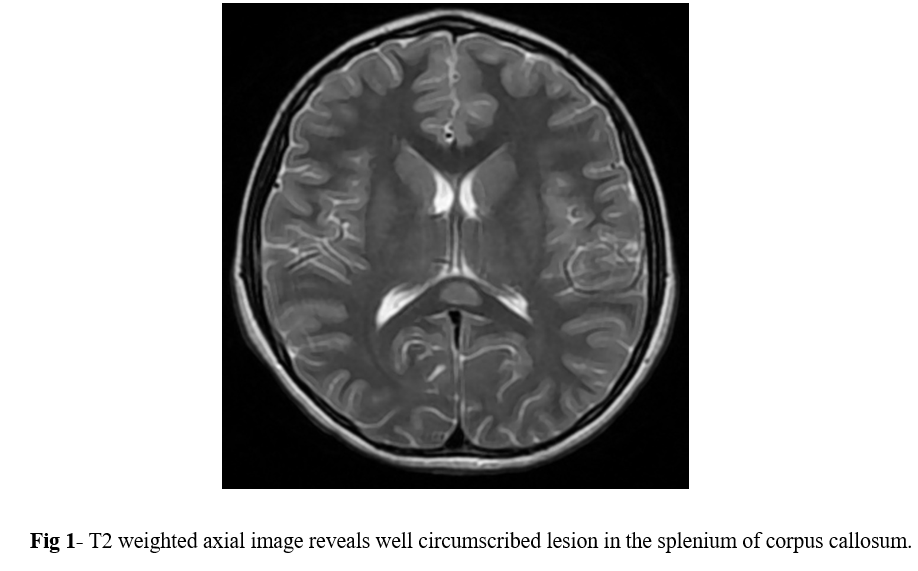
Figure 1
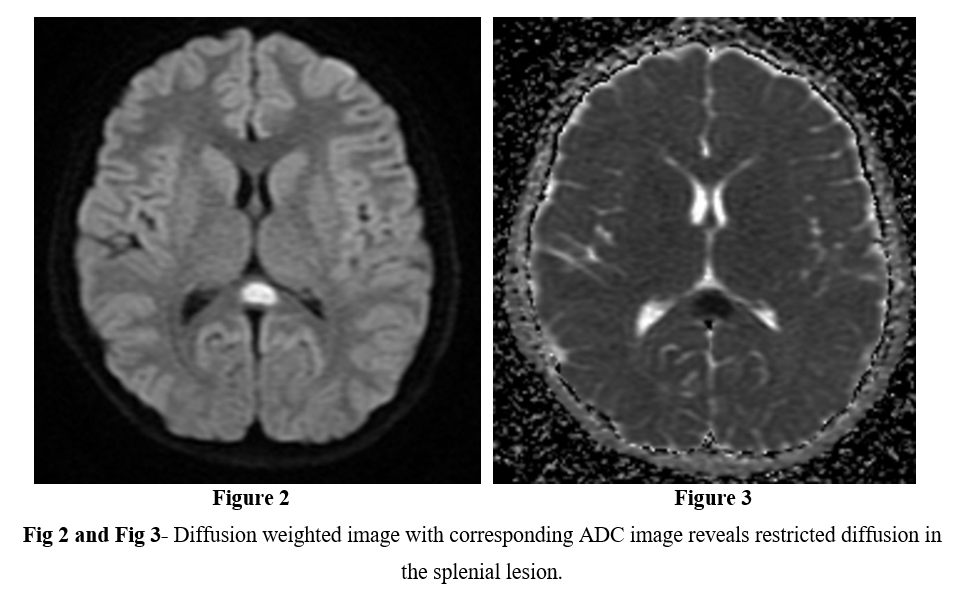
Figure 2
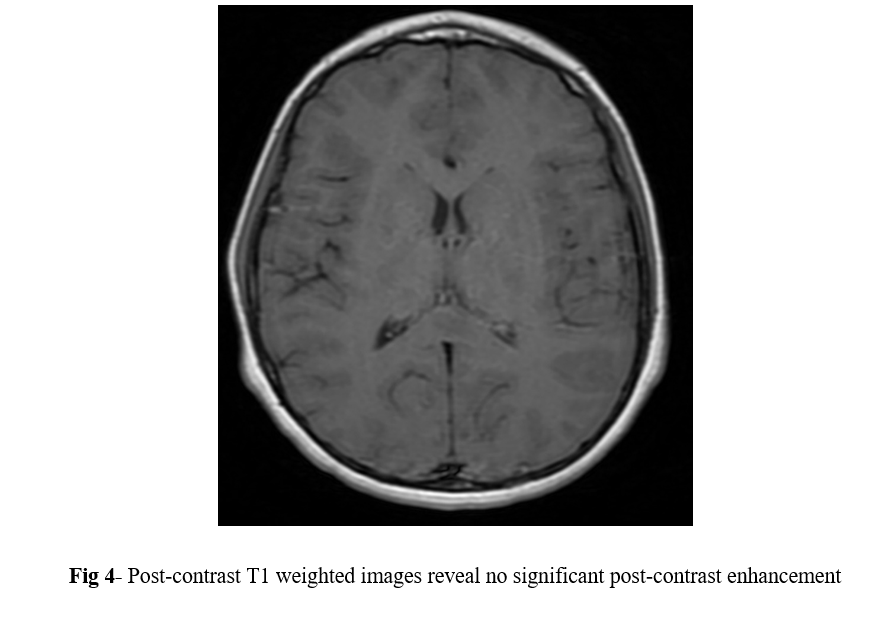
Figure 3
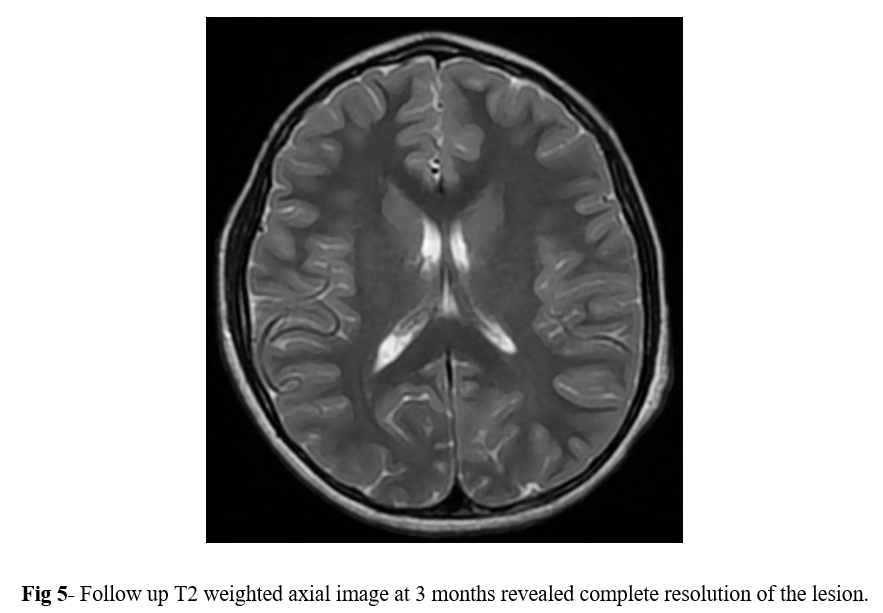
Figure 4